Published on
Urgent message: Immobilization following acute knee injury occurs more commonly than the evidence might dictate in urgent care and other acute care settings. Evaluation of data in existing literature suggest that this common practice carries risk for adverse effects when not warranted.
Matthew Bruce Baird, MD, CAQ-SM; Mallory Shasteen, MD, CAQ-SM; and Vicki Nelson, MD, CAQ-SM.
Citation: Baird MB, Shasteen M, Nelson V. Knee immobilization for acute knee injuries: a review. J Urgent Care Med. 2022;16(8):13-19
ABSTRACT
Context
Immobilization of the knee is commonly used following acute knee injuries despite a paucity of supporting evidence. However, adverse effects of immobilization have been demonstrated. The intent of this review is to stimulate further study on knee immobilization and encourage acute care providers to be judicious with its use.
Evidence Acquisition
This clinical review summarizes the available literature on knee immobilization for acute knee injuries and related articles. Online databases were searched using terms relevant to knee injuries and immobilization (see Methods section further in the article), with pertinent articles extracted and reviewed.
Results
There is a paucity of published evidence on knee immobilization for acute knee injuries.
Conclusions
Available evidence indicates that knee immobilization should be considered for unstable injuries and most fractures. For stable injuries, avoiding use or limiting use to 2 to 3 days with a plan for active early rehabilitation is recommended. Strength of Recommendation Taxonomy: A-B. Keywords: Knee immobilization, knee immobilizers, management of acute knee injuries.
INTRODUCTION
Immobilization of the knee after an acute injury is a common practice in sports medicine clinics, emergency departments, urgent care clinics, and other ambulatory care settings. Benefits include joint stabilization, prevention of further injury, and pain relief. Immobilization is often achieved with a prefabricated knee immobilizer brace, long-leg posterior splint, or less commonly a cylindrical cast. Historically, these modalities have been reserved for postoperative and perioperative management of various knee conditions. Acute care providers, however, quickly adopted the practice for a variety of acute knee injuries.
Despite its common use, there is little evidence supporting rigid knee immobilization; in fact, numerous studies have illustrated its negative consequences, including thigh muscle weakness and atrophy,1-4 loss of motion,5-8 deep-vein thrombosis (DVT),9-11 and delay in return-to-sport or baseline activities.8 A 2020 study by Kilroe, et al suggests that atrophy and weakness are found within the first 2 to 5 days of knee immobilization, suggesting that even very brief periods of immobilization can have adverse effects.2
The purpose of this review is to summarize available literature and recommendations for rigid knee immobilization of acute knee injuries frequently encountered in acute care settings. We discuss use of immobilization for potentially unstable injuries (knee dislocation, patella dislocation, extensor mechanism rupture, tibial plateau fracture, osteochondritis dissecans lesions), and stable injuries (isolated cruciate ligament injuries, meniscus tears, sprains, strains, contusions) separately.
METHODS
PubMed, Medline, Google scholar, and the Cochrane database were utilized to identify the resources for this review. The following keywords were searched:
- Knee immobilization
- Rigid knee immobilization
- Knee splinting.
The following condition-specific phrases were also searched:
- Knee dislocation management
- Patella dislocation management
- Patella fracture management
- Knee extensor mechanism disruption
- Patella tendon rupture management
- Quadriceps tendon rupture management
- Tibial plateau fracture management
- Osteochondritis dissecans management
- Knee sprain management
No temporal restrictions were utilized. Only English language articles were reviewed for inclusion.
At times, the term treatment was substituted for management to identify additional resources. Articles and abstracts identified were reviewed, and those addressing rigid knee immobilization for acute knee injuries were selected. A medical research librarian was consulted to supplement the above literature search.
UNSTABLE INJURIES
Knee Dislocation
Knee dislocation (tibiofemoral dislocation) is a rare, but devastating, knee injury commonly associated with popliteal artery disruption and limb loss. In a 2014 systematic review, Medina reported an 18% incidence of vascular injury after knee dislocation. Of these, 80% underwent surgery with 12% requiring amputation.12 Typically, both cruciate ligaments and one collateral ligament are ruptured, although there are rare cases reporting disruption of a single cruciate ligament after knee dislocation.13-18 About half of knee dislocations are low-energy injuries, typically in the obese, and can be easily missed at initial presentation.19 In addition, half of knee dislocations reduce spontaneously before medical evaluation.20 Thus, acute care providers are encouraged to consider a patient with multiple ligament disruptions to be a result of dislocation, and take great care to consider this injury in the obese with low-energy mechanisms.
Due to the extent of injury seen with knee dislocations, rigid immobilization is often used in the acute setting. The appropriate method of immobilization remains controversial, however. Overall, external fixation is favored over rigid brace immobilization.17,21 Most authors suggest that bracing is the most common initial method, with the following indications for immediate external fixation: open major trauma, vascular injury, compartment syndrome, unstable fracture-dislocation, polytrauma patients requiring operations unrelated to knee injury, and insufficient stability after brace (such as in obese patients).17,22,23 However, aggressive early mobilization protocols are utilized postoperatively with promising outcomes.24-26
For the acute care provider, there are no available studies comparing knee immobilization for acute knee dislocation vs alternative treatment options. Initial rigid immobilization is commonly practiced after knee dislocation, and recommended in order to maximize joint stability, minimize tension across the joint, and reduce pain. Care should be taken to evaluate vascular status before and after bracing to prevent arterial occlusion and distal ischemia. Early mobilization can be considered for postoperative patients.25
Patellar Dislocation
Patellar dislocations make up approximately 3% of acute knee injuries and are the second leading cause of acute knee arthritis behind anterior cruciate ligament (ACL) tears.27,28 Chronic sequelae include early development of patellofemoral osteoarthritis, patellofemoral pain, and chronic instability with recurrent dislocations. Of these, instability and recurrence are the most debilitating consequences, with the incidence of recurrence being around 40%.29 Recurrence rates with surgical vs nonsurgical repair have been found to be quite high with both strategies—10% to 30% in surgical patients, and 13% to 73% in those treated nonsurgically in a small number of limited studies.27,30,31 Most authors favor nonoperative treatment for first-time patellar dislocations in the absence of significant chondral injury with loose body or large osteochondral fracture.
There is debate regarding the decision to immobilize the knee following acute patellar dislocation. Historically, 6 weeks of knee immobilization with a plaster cast has been used.32 Modern recommendations usually include a 2-to-3-week period of immobilization in full extension or 20° of flexion.27,33 Theoretically, this would serve to decrease tension across medial stabilizers (medial patellofemoral ligament and medial retinaculum) and allow fibrosis to begin without disruption. Despite this theoretical advantage, there is no high-quality evidence that immobilization improves outcomes.
A recent, retrospective cohort study of 601 adolescents and young adults with acute patellar dislocation found no difference in recurrence rates between patients treated without immobilization and those treated with 6 weeks of fixed immobilization with gradual increase in range of motion afterwards.34 A small randomized controlled trial (18 patients) showed no difference in recurrence rates between patients treated with taping following 1 week of immobilization in a dorsal splint vs a rigid cast for 5 additional weeks.35 Those patients treated with taping reported improved functional scores at 6 and 12 weeks, and at 5-year follow-up. That same year, however, a conflicting review suggested that a posterior plaster splint might be preferable to a cylindrical cast or brace.36 However, this review only included a single study, and that study did not include a comparison group of patients who were not immobilized.29 Prior to these studies, a 2010 review identified only two prospective randomized controlled trials evaluating immobilization vs no immobilization, with no differences in recurrent dislocation rates found.33
Complications following patella dislocation specifically include quadriceps atrophy and reduced speed of recovery.37 Though current literature is mixed regarding use of immobilization acutely, it is common practice for many providers. There is not adequate evidence available to support or discourage this practice. Thus, we do not recommend providers alter their management recommendations, but do encourage consideration of the risks, benefits, and suspected degree of structural disruption before immobilizing an individual patient. When immobilization is utilized, it is advisable to minimize the duration (1 to 2 weeks). Current data suggest that such a practice would not increase recurrence and would minimize complications.
Patella Fracture and Extensor Mechanism Rupture
Patella fractures make up about 1% of all fractures and are commonly seen in acute care clinics following trauma.38 Typically, urgent surgical reconstruction is required for significantly displaced fractures and fractures associated with extensor mechanism disruption. The goal for the latter group is to obtain surgical fixation within 24 hours of injury.39 The same is true for patellar and quadricep tendon ruptures. Initial management of these injuries with knee immobilization is recommended, ensuring urgent surgical correction.39
Patella fractures not associated with extensor mechanism disruption, however, are treated conservatively with some combination of knee immobilization and physical therapy. Multiple treatment protocols exist, though none have been validated or extensively studied.
There are two older clinical studies with proposed protocols, both of which were summarized and reviewed more recently.38,39 The first, from Bostrom in 1972, included 212 patella fractures with intact extensor mechanisms, <3mm of articular displacement, and <4mm of widening at the fracture site. These injuries were treated nonoperatively with 4 weeks of immobilization in a cylindrical cast. Good or excellent outcomes were reported in 99% of cases at mean 9-year follow-up, with only two treatment failures.38 The second study, by Braun, et al, from 1993 reviewed 40 fractures with intact extensor mechanisms and <1 mm of displacement treated nonoperatively. These patients were immobilized with a posterior splint for 3 to 5 days followed by partial weightbearing and a progressive physical therapy program. At mean follow up of 30.5 months, 80% of patients were pain-free, and 90% had obtained normal range of motion.39 Initial treatment with immediate weightbearing in a hinged knee brace locked in full extension for 1 to 2 weeks is recommended, followed by active-assisted and active range-of-motion exercises, with resistance exercises introduced at 6 weeks.40,41
The limited literature does endorse the safety of nonoperative management for nondisplaced patella fractures with intact extensor mechanisms. Initial knee immobilization with weightbearing has been studied for these injuries and is associated with favorable outcomes. Limiting the duration of immobilization to 1 to 2 weeks is likely safe, particularly for fractures with minimal displacement. Early progression to range-of-motion exercises and resistance exercises under the guidance of a physical therapist is recommended. For injuries with extensor mechanism disruption, rigid immobilization with urgent surgical correction is required.
Tibial Plateau Fracture
Tibial plateau fractures make up another 1% of all fractures.42 Their management depends on the location and degree of displacement, well described by the Schatzker classification system.10,43 Bicondylar and medial tibial plateau fractures are relatively uncommon but considered more severe than lateral tibial plateau fractures. There is general agreement that medial tibial plateau fractures with any displacement should be treated surgically, as precise reduction results in superior functional outcomes.10 Isolated lateral tibial plateau fractures, Schatzker type I, are often treated conservatively. Specific surgical indications for these fractures are controversial, ranging from nonoperative treatment for fractures with up to 1 cm of depression to accepting only minimal depression or displacement prior to surgical fixation44,45 Therefore, close consultation with an orthopedic surgeon is indicated whenever a tibial plateau fracture is diagnosed.
Historically, initial treatment of any tibial plateau fracture has involved knee immobilization. In fractures requiring surgery, there are no trials investigating alternative forms of initial immobilization or level of restriction with regards to patient outcomes. Experts recommend a non-weightbearing status with immediate consultation with orthopedic surgery.46 For those fractures treated nonoperatively, immobilization is typically used for 4 to 8 weeks followed by 8 to 12 weeks of physical therapy.47,48 Very little evidence is available to evaluate this practice. A small cohort study in which 42 patients were treated with 4 to 6 weeks of immobilization in an above-knee plaster cast concluded that outcomes were acceptable in carefully selected patients.48 At 6 months, 76% of patients reported good-to-excellent clinical outcomes. Unfortunately, the authors did not include a surgical group for comparison.
Early open-chain mobilization has been a topic of debate for decades. A small study in 1985 of 112 fractures determined that all patients treated nonoperatively regained full motion when fully immobilized for up to 6 weeks.49 Other authors, however, support the use of early active and passive ROM exercises.49,50 No recent studies are available on this issue.
Most protocols include a period of non-weightbearing with immobilization for 2 to 6 weeks, but there is little evidence to support restricted weightbearing. A 1993 study evaluating lateral tibial plateau fractures found that weightbearing in a cast brace did not produce further depression by more than 2 mm.51 Another small study of postoperative patients in 2018 found that immediate weightbearing did not cause articular collapse or fracture displacement.52 While these conclusions cannot be directly applied to nonoperative patients, it suggests that once the stability of a lateral tibial plateau fracture is established, weightbearing may be reasonable.
Considering historical practices and what little data are currently available, we recommend knee immobilization with a non-weightbearing status for acute management of any tibial plateau fracture along with close consultation with an orthopedic surgeon. Early partial weightbearing may be considered once the fracture has been deemed stable, but is a decision best made by the orthopedic specialist and patient after discussing potential risks. For nondisplaced isolated lateral tibial plateau fractures, open-chain ROM exercises are likely safe, but not standard practice.
Osteochondritis Dissecans
Osteochondritis dissecans (OCD) is another condition for which knee immobilization is often used. The true incidence is poorly understood given the high number of incidental diagnoses, multiple classification systems, and unclear diagnostic criteria.53 Treatment decisions are based on lesion stability (determined by MRI) and the skeletal maturity of the patient. Skeletally immature patients with stable lesions are the subgroup most often treated nonoperatively.54,55 Patients younger than 11 years (far from skeletal maturity) with lesions in the classic location on the lateral border of the medial femoral condyle have the best prognosis.56,57 All other patients should be immobilized in the acute setting and offered surgical fixation. Thus, close consultation with an orthopedic surgeon is critical.
For skeletally immature patients with stable OCD lesions, treatment often includes knee immobilization, bracing, activity restriction, weightbearing restriction, physical therapy, iontophoresis, and extracorporeal shockwave therapy.58 As of 2019, 21 case series and three case reports were found evaluating these modalities with no randomized controlled trials available.58 Analysis of these heterogeneous studies found an overall healing rate of 61.4%. Of the above modalities, only restriction of physical activity has shown consistent correlation with improved outcomes with healing rates between 81% to 96%.58-60 When physical therapy (core and quadricep strengthening) was added to physical restriction, favorable results were also seen with 80% to 90% of asymptomatic patients at mid- and long-term follow-up.61,62 Nine studies looked specifically at knee immobilization with highly variable results; no evidence-based conclusion can be made. Similarly inconclusive reports are seen for weightbearing restrictions.
In summary, for any unstable OCD lesions and for those diagnosed in adults, immediate consultation with orthopedic surgery is indicated with utilization of knee immobilization and weightbearing restrictions until follow-up. For OCD lesions in skeletally immature individuals found incidentally or deemed stable on MRI, we encourage avoiding the use of knee immobilization and treating with activity restriction (avoiding sports, jumping, weighted squats, running, or other impact activities) and low-impact quadricep and core strengthening exercises until instructed otherwise by an orthopedic surgeon or sports medicine physician. Patients should be prepared for a long recovery of approximately 6 months with good treatment compliance.58,63 They should also be informed of the increased risk for developing knee osteoarthritis, with an incidence of 15% seen at 13 years and 30% seen at 35 years after diagnosis.64
STABLE INJURIES
Suspected isolated ligamentous tears, meniscus tears, sprains, and other undifferentiated knee injuries are often treated with knee immobilization by acute care providers. The goal of this practice is to alleviate pain and protect damaged tissue.65 However, this practice can result in muscle atrophy, joint stiffness, weakness, decreased cartilage proteoglycan synthesis, DVT, and decreased bone mass, significantly impairing rehabilitation from injury and delaying surgical intervention when indicated.66,67
Most rehabilitation programs for operative injuries are based on data from studies involving ACL tears. Almost all preoperative ACL treatment protocols include edema control and restoration of motion in preparation for surgery. While no studies found investigated knee immobilization acutely, available data suggest that active rehabilitation protocols including joint mobilization improve postoperative outcomes.68,69 All modern postoperative rehabilitation protocols for cruciate ligament injuries involve early motion with excellent functional outcomes.70-75
While there are few studies investigating rehabilitation programs for meniscus tears, experts agree that knee immobilization is not indicated in the acute setting when meniscus tear is considered likely.76,77 Knee immobilization is commonly utilized postoperatively when attempts at meniscus repair are made (as opposed to meniscal resection).
There are no human trials comparing immobilization with early motion for nonoperative injuries, so most protocols have been extrapolated from animal models. In 2005, Thornton demonstrated impaired healing response with immobilization after MCL injury in rabbits; while an earlier study in dogs by Woo, et al demonstrated improvement in these parameters associated with an early rehabilitation program.77,78 These concepts were used to promote similar rehabilitation protocols in humans.79
Despite the above evidence and expert opinion, knee immobilization continues to be used in the acute treatment of ligamentous, meniscal, and undifferentiated injuries to the knee. A study by Sommerfeldt from 2014 indicated a much higher rate of knee immobilization prescribed by emergency physicians when compared with sports medicine physicians and orthopedic surgeons.80 The most likely reason for this was diagnostic uncertainty.
DISCUSSION
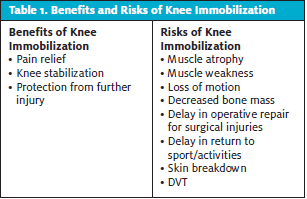
The initial objective of this review was to answer the following clinical question: When should immobilization be used for acute knee injuries? Unfortunately, there are no established evidence-based guidelines to answer this simple question. Animal models, postoperative studies, and dogma have dictated treatment for decades. Above, we have reviewed what evidence is available with regard to knee immobilization to elucidate what current standards of care are based upon. Table 1 summarizes the benefits and risks of immobilization. Each clinical encounter is unique, so we encourage providers to consider and discuss these factors with their patients and families.
Table 2 summarizes management of injuries requiring knee immobilization, which injuries are best managed with early motion and rehabilitation, and highlights those injuries for which further study is needed. For this third category, we feel it is currently reasonable for acute care providers to utilize knee immobilization initially while awaiting further diagnostic information. If used in this setting, however, the duration of knee immobilization should be minimized, as muscle weakness and atrophy can occur quickly. Following immobilization, early range-of-motion exercises, weightbearing, and progression to strength and stability exercises are recommended to expedite recovery and return to baseline activities. We hope that further research can help solidify more evidence-based recommendations, ideally minimizing immobilization to avoid its adverse effects.
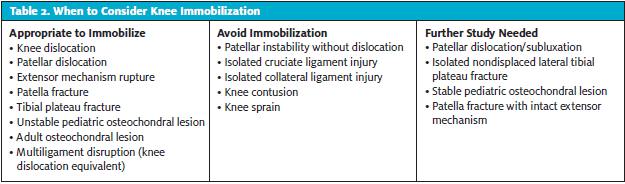
Patellar dislocation/subluxation occurs in more than one category in Table 2. This speaks to the conflicting data published on this injury. It is our contention that injuries associated with patellar instability span a wide range of severities from mild, involving little structural damage (subluxations typically), to severe with bony, chondral, and ligament disruption. Those injuries considered severe often require reduction and/or are associated with a significant hemarthrosis. When utilized, immobilization for 2 weeks is recommended. Less severe injuries, however, with minimal effusion or other objective findings of structural damage or instability, can likely be managed without immobilization. Differentiating between these two entities can be challenging at times, so careful consideration and close collaboration with orthopedic consultants is recommended.
Determining the stability of a knee injury can be challenging in the acute setting, especially when diagnostic uncertainty exists. Improving musculoskeletal assessment skills for nonsurgical providers would certainly help to minimize diagnostic uncertainty and potentially decrease unnecessary utilization of knee immobilization and its adverse effects. When diagnostic uncertainty does occur, collaboration with an orthopedic surgeon is recommended to help avoid or limit duration of knee immobilization.
Ultimately, we hope this review serves to remind acute care providers to strongly consider the risks and benefits of knee immobilization when managing acute knee injuries. While it is often quite easy to apply a prefabricated knee-immobilizing brace or splint, this practice can have adverse effects. While definitive clinical trials have not been published, available evidence indicates that knee immobilization should be used for severe or unstable injuries, and very selectively for more stable injuries.
RECOMMENDATIONS
- For unstable injuries, knee immobilization is indicated.
- For clearly stable injuries, knee immobilization should be avoided in favor of early mobilization and rehabilitation.
- For other or indeterminate injuries, evidence does not support changing standard management; rather, further study is warranted to help target the use of this modality appropriately. Acute care providers should understand the risks of knee immobilization and discuss them with their patients when devising treatment plans.
REFERENCES
- Dirks ML, Wall BT, Van De Valk B, et al. One week of bed rest leads to substantial muscle atrophy and induces whole-body insulin resistance in the absence of skeletal muscle lipid accumulation. Diabetes. 2016;65(10):2862–2875.
- Kilroe SP, Fulford J, Jackman SR, et al. Temporal muscle-specific disuse atrophy during one week of leg immobilization. Med Sci Sports Exerc. 2020 Apr;52(4):944-955
- Suetta C, Frandsen U, Jensen L, et al. Aging affects the transcriptional regulation of human skeletal muscle disuse atrophy. PLoSOne. 2012;7(12):e51238
- Veldhuizen JW, Verstappen FT, Vroemen JP, et al. Functional and morphological adaptations following four weeks of knee immobilization. In J Sports Med. 1993;14(5):283-287.
- Kannus P. Immobilization or early mobilization after an acute soft-tissue injury? Phys Sports Med. 2000;28:55–63
- Kannus P, Parkkari J, Järvinen TLN, et al. Basic science and clinical studies coincide: Active treatment approach is needed after a sports injury. Scand J Med Sci Sports. 2003;13:150–154
- Nash CE, Mickan SM, Del Mar CB, et al. Resting injured limbs delays recovery: a systematic review. J Fam Pract. 2004;53:706–12
- Videman T. Connective tissue and immobilization. Key factors in musculoskeletal degeneration? Clin Orthop Relat Res. 1987Aug;(221):26–32.
- Nameth B, Cannegieter SC. Venous thrombosis following lower-leg cast immobilization and knee arthroscopy: From a population-based approach to individualized therapy. Throb Res. 2019 Feb;174:62-75
- Parkkinen M, Lindahl J, Makinen TJ, et al. Predictors of osteoarthritis following operative treatment of medial tibial plateau fractures. Injury. 2018(49);2:370-375.
- Rasi AM, Safari S, et al. Deep vein thrombosis following below knee immobilization: the need for chemoprophylaxis. Trauma Mon. 2013;Winter;17(4):367-369.
- Medina O. Vascular and nerve injury after knee dislocation: a systematic review. Clin Orthop Relat Res. 2014;472:2621–2629.
- Bratt HD, Newman AP. Complete dislocation of the knee without disruption of both cruciate ligaments. J Trauma. 1993;34:383–389.
- Brautigan B, Johnson DL. The epidemiology of knee dislocations. Clin Sports Med. 2000;19:387–39
- Levy BA, Dajani KA, Whelan DB, et al. Decision making in the multiligament-injured knee: an evidence-based systematic review. J Arthros Rel Surg. 2009;25(4):430-438.
- Maslaris A, Bungartz M, Krettek C, et al. Management of knee dislocation prior to ligament reconstruction: Update of a universal treatment algorithm. Euro J Orthop Surg Traumatol. 2018;28(6):1001-1015.
- Shelbourne KD, Pritchard J, Rettig AC, et al. Knee dislocations intact PCL. Orth Rev. 1992;21(5):610–611.
- Georgiadis A, Mohammed FH, Mizerik K, Nypaver TJ. Changing presentation of knee dislocation and vascular injury from high-energy trauma to low-energy falls in the morbidly obese. J Vasc Surg. 2013;57(5):1196-1203.
- Seroyer ST, Musahl V, Harner CD. Management of the acute knee dislocation: the Pittsburgh experience. Injury. 2008;39(7):710-718.
- Levy BA, Fanelli GC, Whelan DB, et al. Controversies in the treatment of knee dislocations and multiligament reconstruction. JAAOS. 2009;17:197–206.
- Fanelli GC. Knee dislocation and multiple ligament injuries of the knee. Sports Med Athroscop Rev. 2018;26(4):150-152.
- Fanelli GC, Fanelli DG. Multiple ligament knee injuries. J Knee Surg. 2018;31(5):399-409.
- Marcacci M, Zaffagnini S, Bonanzinga T, et al. Surgical technique: articulated external fixator for treatment of complex knee dislocation. Colin Orthop Relat Res. 2012;470(3):869–876.
- Stannard JP, Nuelle CW, McGwin G, Volgas DA. Hinged external fixation in the treatment of knee dislocation: a prospective randomized study. JBJS. 2014;96:184–191.
- Zaffagnini S, Iacono F, Presti M, et al. A new hinged dynamic distractor, for immediate mobilization after knee dislocations. Arch Orthop Trauma Surg. 2008;128:1233-1237.
- Duthon VB. Acute traumatic patellar dislocation. Orthop Traumatol Surg Res. 2015;10(1 Suppl):S59-67.
- Stefancin JJ, Parker RD. First time traumatic patellar dislocation: a systematic review. Clin Ortho and Rel Res. 2007;45:93-101.
- Maenpaa H, Lehto MU. Recurrence after patellar dislocation. Redislocation in 37/75 patients followed for 6–24 years. Acta Orthop Scand. 1997;68(5):424–426.
- Nwachukwu BU, Schairer WW, Green DW, Dodwell ER. Surgical versus conservative management of acute patellar dislocation in children and adolescents: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2016;24(3):760-767.
- Regalado GR, Kokki H, Kroger H, et al. Six-year outcome after non-surgical versus surgical treatment of acute primary patellar dislocation in adolescents: a prospective randomized trial. Knee Surg Sports Traumatol Arthrosc. 2016; 24:6–11.
- Hughston JC. Subluxation of the patella. JBJS 1968;50:1003–1026
- Smith TO, Donell ST. Immobilization regime following lateral patellar dislocation: a systematic review and meta-analysis of the current evidence base. Eur J Trauma Emerg Surg. 2010;36(4):353-360.
- Kaewkongnok B, Milandt N, Møllenborg C, et al. Does different duration of no-operative immobilization have an effect on redislocation rate of primary patellar dislocation? A retrospective multicenter cohort study. The Knee. 2018;25(1):51-58.
- Rood A, Boons H, Ploegmakers J, et al. Tape versus cast for non-operative treatment of primary patellar dislocation: a randomized controlled trial. Arch Orthop Trauma Surg. 2012;132, 1199–1203.
- Van Gemert JP, Hessels R, Gakeer MI. Patellar dislocation: cylinder cast, splint, or brace? An evidence-based review of the literature. Int J Emerg Med. 2012;5:45
- Kiviluoto O, Pasila M, Santavirta S, et al. Recurrence after conservative treatment of acute dislocation of the patella. Ital J Sport Traumatol. 1986;3:159–162.
- Bostrom A. Fracture of the patella: a study of 422 patellar fractures. Acta Ortho Scandin. 1972;143:1-80.
- Braun W, Rüter A, Kundel K, Kolbinger S. Indications and results of nonoperative treatment of patellar fractures. Clin Orthop Relat Res. 1993;(289):197-201.
- Bui CN, Scolaro JA. Treatment of patellar fractures and injuries to the extensor mechanism of the knee: a critical analysis review. JBJS Rev. 2018 Oct;6(10):e1.
- Melvin JS, Mehta S. Patellar fractures in adults. JAAOS. 2011;19(4):198-207.
- Court-Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury. 2006;37:691–697.
- Schatzker J, McBroom R, Bruce D. The tibial plateau fracture: the Toronto experience 1968-1975. Clin Orthop. 1979;138:94-104.
- Burri C, Bartzke G, Coldwey J, et al. Fractures of the tibial plateau. Clin Orthop. 1979;138:84-93.
- Koval KJ, Helfet DL. Tibial plateau fractures: evaluation and treatment. JAAOS. 1995(3);2:86-94.
- Court-Brown C, McQueen MM, Tornetta III P. Trauma. Philadelphia: Lippincott Williams & Wilkins 2006: 322-339.
- Robertson GA, Wong SJ, Wood AM. Return to sport following tibial plateau fractures: a systematic review. World J Orthop.2017;8(7):574-587.
- Shrestha R, Kandel M, Gupta H, et al. A study of conservative management of tibial plateau fractures. J Coll Med Sci-Nepal. 2016;12(1):5-9.
- Gausewitz S, Hohl M. The significance of early motion in the treatment of tibial plateau fractures. Clin Orthopaed Rel Res. 1985;202:135-138.
- Moore TM, Patzakis MJ, Harvey JP. Tibial plateau fractures: definition, demographics, treatment rationale, and long term results of closed traction management or operative reduction. J Orthop Trauma. 1987;1(2):97-119
MORE REFERENCES
- Segal D, Mallik AR, Wetzler MJ, et al. Early weight bearing of lateral tibial plateau fractures. Clin Orthopaed Rel Res. 1993;294:232-237.
- Williamson M, Iliopoulos E, Jain A, et al. Immediate weight bearing after plate fixation of fractures of the tibial plateau. Injury. 2018;49(10):1886-1890.
- Chamber HG, Shea KG, Carey JL. AAOS Clinical Practice Guideline: diagnosis and treatment of osteochondritis desiccant. J Am Acad Orthop Surg. 2011;19(5):307-309.
- Pacual-Garrido C, Moran CJ, Green DW, et al. Osteochondritis dissecans of the knee in children and adolescents. Curt Opin Pediatr. 2013;25:46-51
- Wall EJ, Vourazeris J, Myer GD, et al. The healing potential of stabile juvenile osteochondritis dissecans knee lesions. JBJS. 2008;90:2655-2664.
- Bauer KL, Polousky JD. Management of osteochondritis desiccant lesions of the knee, elbow, and ankle. Clinics in Sp Med. 2017;36(3):469-487.
- Weiss JM, Nikizad H, Shea KG, et al. The incidence of surgery in osteochondritis dissecans in children and adolescents. Orthop J Sports Med. 2016;4:1-7.
- Andriolo L, Candrian C, Papio T, et al. Osteochondritis dissecans of the knee – conservative treatment strategies: a systemic review. Cartilage. 2019;10(3):267-277.
- de Gauzy SJ, Mansat C, Darodes PH, Cahuzac JP. Natural course of steochondritis dissecans in children. J Pediatr Orthop B. 1999;8(1):26-28.
- Yoshida S, Ikata T, Takai H, et al. Osteochondritis dissecas of the femoral condyle in the growth stage. Colin Orthop Relat Res. 1998;346:162-170.
- Hughes JA, Cook JV, Churchill MA, Warren ME. Juvenile osteochondritis dissecans: a 5-year review of the natural history using clinical and MRI evaluation. Pediatric Radiol. 2003;33(6):410-417.
- Hughston JC, Hergenroeder PT, Courtenay BG. Osteochondritis dissecans of the formal condyles. JBJS Am. 1984;66(9):1340-1348.
- D’Angelo K, Kim p, Murnaghan ML. Juvenile osteochondritis dissecans in a 13-year-old male athlete: a case report. J Can Chiropr Assoc. 2014;58(4):384-394.
- Sanders TL, Pareek A, Johnson NR, et al. Nonoperative management of osteochondritis dissecans of the knee: progression to osteoarthritis and arthroplasty at mean 13-year follow-up. Orthop J Sports Med. 2017;5(7):2325967117704644.
- Gravlee JR, Van Durme DJ. Braces and splints for musculoskeletal conditions. Am Fam Physician. 2007;75:342-348.
- Millett PJ, Wickiewicz TL, Warren RF. Motion loss after ligament injuries to the knee: part i: causes. Am J Sports Med. 2001;29:664-675.
- Millett PJ, Wickiewicz TL, Warren RF. Motion loss after ligament injuries to the knee part II: prevention and treatment. Am J Sports Med. 2001;29:822-828 .
- Shelbourne KD, Wilckens JH, Mollabashy A, et al. Arthrofibrosis in acute anterior cruciate ligament reconstruction. The effect of timing of reconstruction and rehabilitation. Am J Sports Med. 1991;19:332-336.
- Wilk KE, Arrigo CA. Rehabilitation principles of the anterior cruciate ligament reconstructed knee. Clin in Sp Med. 2017;36(1):189-232.
- De Carlo MS, McDivitt R. Rehabilitation of patients following autogenic bone-patellar tendon-bone ACL reconstruction: a 20-year perspective. N Am J Sports Phys Ther. 2006;1:108-123.
- Kim SJ, Kumar P, Oh KS. Anterior cruciate ligament reconstruction: autogenous quadriceps tendon-bone compared with bone-patellar tendon-bone grafts at 2-year follow-up. Arthroscopy. 2009;25:137-144.
- Mariani PP, Santori N, Adriani E, et al. Accelerated rehabilitation after arthroscopic meniscal repair: a clinical and magnetic resonance imaging evaluation. Arthroscopy. 1996;12:680-686.
- Vanwanseele B, Lucchinetti E, Stussi E. The effects of immobilization on the characteristics of articular cartilage: current concepts and future directions. Osteoarthritis Cartilage. 2002;10: 408-419.
- Wilk KE. Rehabilitation of isolated and combined posterior cruciate ligament injuries. Clin Sports Med. 1994;13:649-677.
- Wilk KE, Reinold MM, Hooks TR. Recent advances in the rehabilitation of isolated and combined anterior cruciate ligament injuries. Orthop Clin North Am. 2003;34:107-137.
- Singhal M, Patel J, Johnson D. Knee: medial ligament injuries. In: DeLee JC, Drez D Jr, Miller MD, eds. DeLee and Drez’s Orthopaedic Sports Medicine. 3rd ed. Philadelphia (PA): Saunders; 2009.
- Thornton GM, Johnson JC, Maser RV, et al. Strength of medial structures of the knee joint are decreased by isolated injury to the medial collateral ligament and subsequent joint immobilization. J Orthop Res. 2005;23:1191–1198.
- Woo SL, Gomez MA, Seguchi Y, et al. Measurement of mechanical properties of ligament substance from a bone-ligament-bone preparation. J Orthop RES. 1983;1:22-29.
- Wijdicks CA, Griffin CJ, Johansen SM, et al. Injuries to the medical collateral ligament and associated medial structures of the knee. JBJS. 2010;92(5):1266-1280.
- Sommerfeldt M, Bouliane M, Otto D, et al. The use of early immobilization in the management of acute soft-tissue injuries of the knee: results of a survey of emergency physicians, sports medicine physicians and orthopedic surgeons. Can J Surg. 2015 Feb;58(1):48-53.
Author affiliations: Matthew Bruce Baird, MD, CAQ-SM,Department of Emergency Medicine and Orthopedics, Prisma Health – Upstate; University of South Carolina – Greenville School of Medicine. Mallory Shasteen, MD, CAQ-SM, Department of Emergency Medicine, Prisma Health – Upstate. University of South Carolina – Greenville School of Medicine. Vicki Nelson, MD, CAQ-SM, Department of Family Medicine, Prisma Health – Upstate. University of South Carolina – Greenville School of Medicine. The authors have no relevant financial relationships with any commercial interests.
Read More on the Knee
- Evaluation Of Knee Pain: An Urgent Care Approach
- A 17-Year-Old Male With Knee Pain After A Fall
- A 47-Year-Old Male With Knee Pain And Swelling After A Fall