Published on
Urgent message: Use of a finger tourniquet can ensure a bloodless field when performing laceration repair to fingers and toes, thereby reducing risk for damage to underlying vital structures and increasing the prospects for positive outcomes.
Patrick O’Malley, MD
After repairing scores of finger lacerations over the years, I have learned there are a few essential supplies required for these cases; the most critical among them, however, is the finger tourniquet. This simple device makes a world of difference when closing finger (and toe) lacerations.
We’ve all experienced how the fingers have a rich blood supply and can bleed profusely. Combined with the fact that so many patients are on agents that affect coagulation, the reason a finger tourniquet must be in your digital laceration tool kit should be clear. A field obscured by actively oozing blood creates a nearly impossible situation for fully evaluating the presence of joint capsule or tendon injury and foreign body. The “bloodless field” improves precision in repair and reduces risk of inadvertently damaging underlying vital structures such as tendons or violating the joint capsule during repair.1,2
When it comes to a tourniquet, there are many options to choose from. While there are many commercial products available, other methods of tourniquet creation can be used with readily available supplies.
IMPROVISED TOURNIQUETS
One improvised tourniquet approach is the glove technique. To perform this, have the patient put a glove on the affected hand, cut a small hole at the tip of the affected finger and roll the rest of the material down to the base of the finger while the fingers are pointed up. This will constrict the base of the finger, thereby acting as a tourniquet. (See Figure 1.)

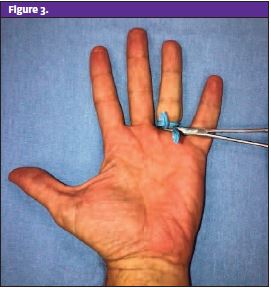
As with commercially available products, the glove technique acts to exsanguinate the finger as the glove material is being rolled down the finger. It also keeps the hand covered, reducing the risk of cross-contamination as the hand is now covered by the glove. Ensure an appropriate glove size is used so rolling the material down the finger does not generate too much pressure, resulting in potential nerve injury. Another method for an ad hoc tourniquet involves the use of a standard IV tourniquet or the elastic band from the wrist of a disposable glove. To perform this technique, wrap the elastic material around the finger and hold it in place with a hemostat. See Figure 2 and Figure 3.)

With a little practice, you can determine which of these materials and approaches seems the easiest for you within your clinical setting.
TIPS
It should be noted that a digital block is best performed prior to tourniquet application, regardless of the method you use.
When applying the tourniquet, it’s also important that it be pushed as proximally as possible (ideally to the base of the finger at the webspace). This will create a near-bloodless field, allowing for better visualization of the wound itself so you can actually see the suture needle going through the tissue.
Finger tourniquets are not without potential problems. Once the repair is complete, make sure to remove the tourniquet promptly. Remarkably, there have been cases of patients being sent home after a finger procedure with the tourniquet left on, likely because the finger was anesthetized and a medical assistant dressed the wound. Needless to say, in these cases the finger is at serious risk of irreparable ischemic injury.3,4
Furthermore, the amount of pressure generated by these devices and techniques is variable and can reach upwards of 600 mmHg—enough to cause significant nerve damage. You must be familiar with this and be sure to not use a device or technique that will lead to this potentially disastrous complication.5,6
SUMMARY
Whether it be with an improvised or commercial tourniquet, try using one on your next finger laceration. Once you give it a shot, you’ll never repair a wounded digit without one again. Just remember to remove the tourniquet and to avoid applying too much pressure to avoid nerve injury.
References
- Bowen WT, Slaven EM. Evidence-based management of acute hand injuries in the emergency department. Emerg Med Pract. 2014;16(12). Available at: https://www.ebmedicine.net/media_library/files/1214%20Hand%20Injuries(1).pdf. Accessed April 11, 2022.
- Brancato JC. Minor wound evaluation preparation for closure. In: UpToDate. Stack AM, ed. UpToDate. Waltham, MA. Available at: https://www.uptodate.com/contents/minor-wound-evaluation-and-preparation-for-closure. Last updated December 1, 2021. Accessed April 11, 2022.
- Avci G, Akan M, Yildirim S, Akӧz T. Digital neurovascular compression due to a forgotten tourniquet. Hand Surg. 2003;8(1):133-136.
- de Boer HL, Houpt P. Rubber glove tourniquet: perhaps not so simple or safe? Eur J Plastic Surg. 2007;30:91-92.
- Lamont T, Watts F, Stanley J, et al. Reducing risk of tourniquets left on after finger and toe surgery: summary of a safety report from the National Patient Safety Agency. BMJ. 2010;340:c1981.
- Lahham S, Tu K, Ni M, et al. Comparison of pressures applied by digital tourniquets in the emergency department. West J Emerg Med. 2011;12(2):242-249.
Patrick O’Malley, MD is an emergency physician at Newberry County Memorial Hospital, Newberry, SC.