Published on
Urgent message: Injuries caused by pressure washers often require debridement or, in severe cases, amputation. Immediate assessment and appropriate management, where feasible, can preclude the need for surgical intervention while effecting a positive outcome.
Ellen Hancock, MD; Julie Park; MD, FACS; and Kendall Wermine
INTRODUCTION
Pressure washer injuries tend to involve the lower extremities and abdomen and usually require a form of surgical intervention such as debridement of tissue and, in severe cases, amputation.1-4 The need for surgical intervention is heightened when inorganic compounds are present in the wound.5 Here, we present a case of a pressure washer injury to the hand that was resolved without surgical intervention.
CASE PRESENTATION
An otherwise healthy 34-year-old male presented with a small laceration and edema to the middle and right fingers on his right hand, sustained while trying to fix a pressurized power washer that he had been using on his driveway that morning. The power washer contained just water and oxygen, with no other chemicals.
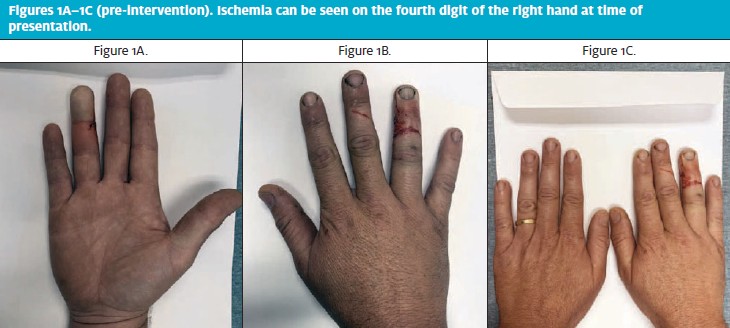
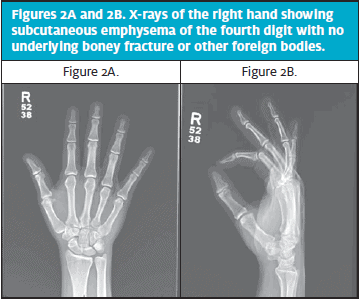
Upon initial examination, the distal portion of the ring finger was numb to sensation, ischemic, and white (Figure 1). Crepitus was palpated volarly and dorsally in the palm and dorsum; slight edema was noted on the right ring finger. Superficial lacerations to the volar and radial fourth digit and dorsal third digit were also present. An x-ray taken to rule out underlying boney fracture revealed subcutaneous emphysema of the fourth digit and lack of other foreign bodies (Figure 2). Physical examination of the finger showed the patient had full extension capabilities of his digits and only the last 10% of flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) flexion was limited due to pain and stiffness.
The fact that water and oxygen were the only substances present in the wound allowed for a treatment method that avoided surgery. Treatment consisted of physically milking the water and air bubbles out of the wound while also using a warm compress along with antibiotics. This was accompanied by elevation of the right hand. Water and oxygen were milked out of the wound until no more water or air bubbles exited the wound through the laceration, which took approximately 30 minutes. Sensation, blood flow, and color returned to the finger, as evidenced through physical exam and Doppler (Figures 3A–3C). The patient was ultimately admitted to the hospital, but maintained full range of motion and did not require surgical intervention.

DISCUSSION
Much of the current literature cites pressure washer injuries as occurring to the lower extremities and the abdomen.1,2 Three cases of lower extremity injuries all required debridement.1 Even though these types of injuries have become more common, very few cases involve the hands.1-4
This case shows a new way to treat pressure washer injuries to the hands. The patient had a combination of water and air bubbles in the wound. These were able to be massaged out and in combination with elevating the patient’s hand and using a warm compress, surgical intervention was avoided. No inorganic substances were present in the wound, which made this method of treatment possible. The patient was prescribed a 7-day course of doxycycline and ciprofloxacin, in cases of pressure washer injuries broad spectrum antibiotics are normally utilized.6
A method similar to the one described in this case was utilized in a case by Kon, et al,7 where surgical intervention was not used for a patient with a high-pressure injury to the hand. Instead, they elevated the patient’s hand and used antibiotics to treat the patient. The patient had a few complications, such as swelling of the small finger, but after treatment the patient left the hospital with normal functioning of all digits. Surgical intervention could be avoided because only nonsterile water had entered the wound.7
It is important to note that this method of elevation and massage therapy is not viable in every washer pressure injury, even if water is the only substance to enter the wound. Ray and Rainsburywrote about a high-pressure injury from a steam hose that affected the foot of the patient. The injury resulted in burns and ended with digital amputation.8 Typically, in hand cases with involvement of the tip of the index finger and the thumb, restoration of the tip sensation by a sensate flap would need to be considered along with regular follow-up and early intensive rehabilitation to achieve optimal functional outcome.5 We were able to avoid these complications and others such as loss of finger, loss of flexor tendons, loss of range of motion, stiffness, longer recovery, and flexor tenosynovitis.
In cases where inorganic material such as sand or paint enters the wound, the treatment method used in this case is not practical as the material that entered the wound will require irrigation and debridement for removal.9 X-ray in this type of injury when substances other than water and air are involved shows the quantity and distribution of radio-opaque fluids6; the x-ray for this patient showed subcutaneous emphysema of the fourth digit with no underlying boney fracture or other foreign bodies.
Fracture is not typical for high pressure injuries, with few documented cases of fracture caused by high pressure water jets.1
This case shows the utility of nonsurgical intervention when treating a pressure washer injury to the hand. By massaging out the air bubbles and water that filled the finger, normal blood flow was returned, and the patient was able to avoid surgery, and be discharged without permanent hyperesthesia, continuous pain, cold intolerance, contracture, or reduced sensitivity which are common after high-pressure injury.6
CONCLUSION
Pressure washer injuries to the hand, though atypical, usually require surgical intervention. In this case, in which only water and oxygen were injected into the patient’s wound, a novel treatment plan proved effective in avoiding surgery and facilitating quicker haling time.
REFERENCES
- Connolly CM, Munro KJG, Hogg FJ, Munnoch DA. Water-power: High pressure water jets and devastating lower limb injury. J Plast Reconstr Aesthet Surg. 2010;63(3):E327-E328.
- Kesse Bl, Eilam D, Ashkenazi I, Alfici R. Severe hydroblast intra-abdominal injuries due to high-pressure water jet without penetration of abdominal cavity. Injury Extra. 2005;36:82–83.
- Harvey RL, Ashley DA, Yates L, et al. Major vascular injury from high-pressure water jet. J Trauma. 1996;40:165-167.
- Neil RW, George B. Penetrating intra-abdominal injury caused by high-pressure water jet. BMJ. 1969;2:357-358.
- Saraf S. High-pressure injection injury of the finger. Indian J Orthopaed. 2012;46(6):725.
- Verhoeven N, Hierner R. High-pressure injection injury of the hand: an often underestimated trauma: case report with study of the literature. Strategies Trauma Limb Reconstr. 2008;3(1):27-33.
- Kon M, Sagi A. High-pressure water jet injury of the hand. J Hand Surg. 1985;10:412–414.
- Ray SA, Rainsbury RM. High pressure industrial steam washer injury resulting in digital amputation. Burns. 1992;18:256.
- Gillespie CA, Rodeheaver GT, Smith S, et al. Airless paint gun injuries: Definition and management. Am J Surg. 1974;128:383–391.
Author affiliations: Ellen Hancock, MD, Department of Surgery, University of Texas Medical Branch at Galveston. Julie E. Park, MD, FACS, Department of Surgery, University of Texas Medical Branch at Galveston. Kendall Wermine, School of Medicine, University of Texas Medical Branch at Galveston. The authors have no relevant financial relationships with any commercial interests.