Published on
Urgent message: Tissue adhesives are quick, painless, and result in a good cosmetic outcome, making them well-suited for use to treat wounds in urgent care.
SIMON TANKSLEY, M.D.
Introduction
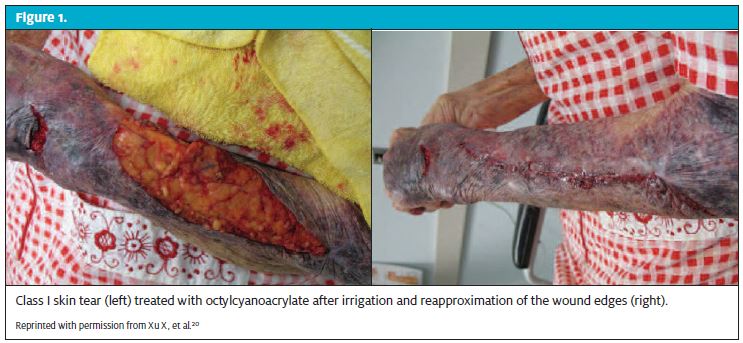
Tissue adhesives are ideal for closing simple lacerations, especially on the face of children.1-3 Such repairs are quick, painless, and do not require removal of sutures. They are also excellent for treating large skin tears in the elderly (Figure 1) and particularly useful for thin, fragile skin because unlike sutures, the adhesives do not tear through the tissues or strangulate them.4 Tissue adhesives are also a needless method of wound repair that eliminates the chance of a needle-stick injury.5 In the last 20 years, numerous studies have proven that, when used appropriately, the 3-month cosmetic appearance of wounds treated with tissue adhesives is equivalent to that of sutures. 6-12 It has also been shown that tissue adhesives are faster to apply and quicker to attain proficiency in than sutures. 7-13
Most tissue adhesives are based on cyanoacrylate, the active ingredient in superglue. The mechanism of action of cyanoacrylate is a polymerization process rather than an evaporative process. On contact with anionic substances, such as blood or moisture on the skin, cyanoacrylate changes from a monomer to a polymer forming a solid film that holds the apposed wound edges together. Several different formulations of tissue adhesives have been marketed in the last 40 years, including butylcyanoacrylate marketed under the His toacryl®, Indermil®, PeriAcryl® and LiquiBand® brand names. The most popular formulation used today is 2- octylcyanoacrylate, also known as Dermabond® or SurgiSeal®. This article reviews factors to take into account when considering use of tissue adhesives, technique for application, aftercare, tips for troubleshooting and billing for such repairs.
Choosing A Wound Closure Method
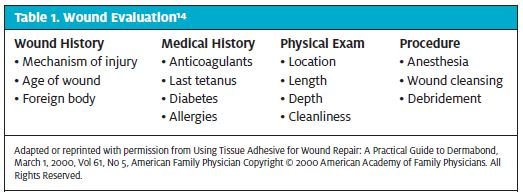
Numerous factors must be considered when choosing a wound closure method. Table 1 summarizes the most important factors to take into account when evaluating a wound.14
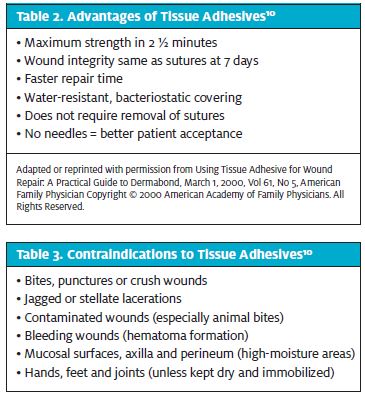
The advantages and disadvantages of tissue adhesives are summarized in Tables 2 and 3. When any of the conditions in Table 2 are present, tissue adhesive should be considered. However, the presence of any factors listed in Table 3 should be seen as a contraindication for the use of tissue adhesives. For example, for a 3-year-old with a simple chin laceration, tissue adhesive would be ideal because the repair time is fast, it affords a water-resistant covering, and there is no need for a traumatic procedure and or subsequent removal of sutures. In contrast, for an adult with a finger laceration who washes dishes at work, sutures would be best because dishwashing is a high-tension and high moisture environment.
Many studies have demonstrated that tissue adhesive is equivalent in strength to a 4-0 nylon suture.15-17 In my professional experience, however, I have found it best to limit use of tissue adhesives to wounds that might otherwise have required a 5-0 nylon suture in order to minimize the risk of dehiscence.
Actively bleeding wounds present two challenges to using tissue adhesive. First, bleeding must be controlled to allow the tissue adhesive adhere to the skin. I have found that tissue adhesive polymerizes instantly on contact with blood, which prevents it from adhering to the skin. The second problem is hematoma formation, which I have seen in one patient on warfarin who had a skin tear on the forearm. On the day of the repair, the wound was hemostatic. She returned the next day with a large hematoma underneath the skin that had to be drained. On the third day, the hematoma was small but did not require drainage.
Accurate approximation of the lacerated edges of the dermis is the most crucial step in attaining the best cosmetic outcome with tissue adhesives. It is at this layer that collagen is generated, resulting in healing and closure of the gap in the wounded skin. Thus, a single, linear laceration from a sharp object would be a good candidate for repair with tissue adhesive, whereas a stellate laceration from a crush injury is best sutured because the operator can use different suturing techniques to perfectly match each side of the torn dermal layer.
Whether a wound is clean, clean contaminated, contaminated or dirty must also be considered. Most of the wounds encountered in the urgent care setting will be either clean contaminated or contaminated. Tissue adhesives should never be used to close contaminated or dirty wounds such as animal bites or road abrasions. Stellate lacerations have ragged, devitalized wound edges that are at increased risk of infection due to tissue necrosis and should not be closed with a tissue adhesive. The decision whether or not to close a clean contaminated wound with tissue adhesive is based on clinical judgment. One study found that, assuming cleansing and preparation are equal, wounds closed with tissue adhesives have lower bacterial counts than wounds closed with sutures.18
That is believed to be due to the antimicrobial properties of the polymer. However, if wound cleansing and preparation are abbreviated, which often happens because of the ease of use of tissue adhesive, an increase in infection rate does occur.10 The size and age of the wound are the last factors to take into account. While most clinicians are not comfort- able closing large lacerations with tissue adhesives, there is evidence that is an acceptable practice. A study of 209 patients with lacerations with a mean length of 16 cm (range 4-69 cm) found that high-viscosity tissue adhesive provided epidermal wound closure equivalent to that of other sutures with a trend of decreased incidence of wound infection.19 Another case report showed that tissue adhesive can be used to close a very large skin tear on the dorsum of the forearm of an elderly person.21 Despite this, most clinicians are not comfortable with closing large lacerations and agree that tissue adhesive should not be used for lacerations on high-tension areas of the body such as the lower leg. One group of plastic surgeons recommends that tissue adhesives be used for lacerations 4 cm and smaller.20 Lastly, although there is no available literature, most clinicians would agree that wounds over 24 hours old should not be closed using tissue adhesives. One small study found that skin tears of all types treated within 8 hours after injury including very large one scan be safely closed using topical adhesive.22
Application
Using tissue adhesives is significantly quicker than using sutures. The manufacturer’s product information provides step-by-step instructions for application.23 One study found that time in a pediatric emergency department was reduced from 106 minutes to 69 minutes by using tissue adhesive instead of sutures The most important thing when using tissue adhesives is to not allow the glue to enter into the wound or dribble to important structures near the wound, such as the eye. Two studies have definitively shown that interposing glue into the wound results in greater scarring.2,24 Techniques to avoid migration of tissue adhesive into the eye are discussed in the troubleshooting section of this article.
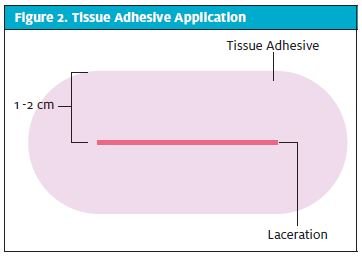
Tissue adhesive should be applied so that there is 1 to 2 cm of width on either side of the laceration, as shown in Figure 2. This is very important because the most common cause of tissue adhesive failure is substrate failure. Increasing the area that the tissue adhesive is in con- tact with skin can minimize substrate failure. One exception to this rule is when using tissue adhesive on a finger. To prevent it from acting as a constricting band, care should be exercised to ensure that adhesive is not applied circumferentially around the finger.
When using tissue adhesives on children, it is also good to be cognizant that the polymerization reaction causes heat to be released. Most adults have thicker skin and will not notice this, however, occasionally young children may become scared when they feel the adhesive become warm.3 This usually lasts no more than 2 to 3 seconds. Also, because tissue adhesive works by a polymerization process and not an evaporative process, blowing air on the liquid adhesive will not make it polymerize any faster and doing so risks causing contamination from spewed saliva.
It is also advisable to avoid references to tissue adhesives as “superglue” in front of patients or parents. One case report found that a parent, trying to save money, applied superglue to his child’s wound thinking it was the same thing as tissue adhesives. Superglue polymerizes much faster than tissue adhesives and actually caused significant first-degree burns to the child in the case report.25 Thus, clinic staff should be careful to avoid using the term “superglue” when referring to tissue adhesives.
Aftercare
Tissue adhesive films form excellent microbial barriers and are effective in protecting wounds from external bacterial invasion and reducing bacterial contamina- tion.26,27 Because tissue adhesives form their own water- proof, antimicrobial barrier, no additional dressings are required.28 Most tissue adhesive manufacturers recom- mend not soaking the film and only letting it get wet briefly in the shower. While this is reasonable, a study found that exposure of tissue adhesive to daily soaking in warm, soapy water for an hour at a time shortens the sloughing time by only 1 day (5.2 to 4.2 days).29 It is important to emphasize to the patient not to apply antibiotic ointment to the wound, as that will dissolve the tissue adhesive.
Troubleshooting
The main challenge of applying tissue adhesive is its tendency to migrate away from the wound site. Newer high-viscosity tissue adhesives are less likely to migrate than older, lower-viscosity tissue adhesives.30 Currently, Dermabond Advanced® is the most viscous tissue adhesive available and has been shown to migrate the least distance from the wound site.31 However, even when using high-viscosity tissue adhesive, special care should be taken when working in proximity to the eyes to avoid inadvertent tarsorrhaphy.32 Placing the patient in the Trendelenburg position before repairing lacerations above the eyes can prevent runoff into the eyes.
Migration of glue into the eye. If the eyes are inadvertently glued closed, that can easily be fixed with repeat- ed application of a petroleum-based ointment such as bacitracin to speed up the breakdown process. Tissue adhesive can also be removed using silver sulfadiazine, but that should not be used in the eye. Do not force- fully separate the eyelids because that can cause cosmet- ic deformity. If some tissue adhesive inadvertently gets directly onto the cornea or sclera, the first step should be to try and flush it out while it is still liquid, using the eyewash station, but that must be done in less than 10 seconds. If the tissue adhesive has already polymerized prescribe bacitracin ophthalmic ointment to be applied into the affected eye 4 times a day while the patient waits to see an ophthalmologist. Although the patient may be frightened, upset, and have a painful bloodshot eye from the heat released by the polymerization reaction, emergency ophthalmology consult is not necessary. An urgent appointment in 1 to 2 days to remove any remaining tissue adhesive and to evaluate damage to the cornea is adequate. Some tissue adhesives are actually being tested as treatment for corneal abrasions and corneal lacerations.33 However, the author reminds the reader that runoff of tissue adhesive into the eye is preventable.
Another simple method to avoid tissue adhesive migration is to create a wall of bacitracin ointment in the surrounding area. The ointment physically stops the migration of the liquid and also chemically prevents it from binding to the skin to which it is applied. Once the tissue adhesive has polymerized, the ointment should be wiped away from the wound while taking care not to let it come in contact with the polymerized film.
Tissue adhesive failure. There are three types of failure of a tissue adhesive: cohesive, adhesive and substrate failure.34 When failure occurs with tissue adhesives, it is usually due to substrate failure as a result of the adhesive peeling away from the skin surface. It is not usu- ally due to failure of the mechanical properties of the polymer.35 In cases of wound dehiscence, the failure appears to be at the skin-glue interface (substrate failure) rather than because of direct failure of the glue (cohesive failure). One study suggests that skin edges be prepared with alcohol to minimize oil interposition and increase skin adhesion in order to minimize the probability of substrate failure.21
On fingers, rubber bands can be used as tourniquets to control bleeding and allow for easier application. After allowing 60 seconds for the adhesive to polymerize, the tourniquet can be removed. Minimize the chance of blood seepage or hematoma formation by having the patient keep his or her hand elevated above the level of the heart for at least 2 hours.
If a patient returns with a dehisced wound, Steri-Strips® are often all that is needed support the healing wound. If a non-infected wound is not a candidate for healing by secondary intention or use of wound tapes, the laceration to convert into a fresh wound before re- applying tissue adhesive or suturing. Of note, if a child or a developmentally disabled patient removed the tis- sue adhesive, do not re-apply. Support the wound with Steri-Strips® or, if needed, close with sutures.
Allergic reactions. There is clinical evidence that in some cases, use of tissue adhesive can lead to a foreign body reaction.36 One case report showed that a young hair dresser developed an allergic contact dermatitis to two “instant glues” used to attach false hair.37 Another case report was of allergic eyelid contact dermatitis caused by ethylcyanoacrylate containing eyelash adhesive.38
In the arena of wound repair, however, foreign body reaction to tissue adhesive is mitigated if the polymer is not allowed to interpose into the wound. The degradation product of polymerized cyanoacrylate is cyanoacetate and formaldehyde. While it is true that formaldehyde is toxic, the longer alkyl chains of modern tissue adhesives slow degradation, significantly limiting accumulation of byproducts to amounts that can be effectively eliminated by tissues.14 However, tissue adhesive remains con- traindicated in people allergic to formaldehyde.
Reimbursement
Tissue adhesive repair is reimbursed by commercial insurance other than Medicare at the same level as a laceration repair with sutures. When billing for tissue adhesive repair with Medicare, you must use the G0168 code. The G0168 code is a flat rate reimbursement irrespective of the length of the laceration.
Medicare assigns tissue adhesive repair a lower RVU (relative value unit) than suture repair, and thus reimburses at a lower rate, which varies in each state or may not be reimbursed at all. However, if a single laceration is closed with a combination of both sutures and tissue adhesive, the provider can bill for the higher-pay- ing laceration repair CPT code (12001-13160). As with laceration repair with sutures, location, length, and depth must be documented. Billing for multiple lacerations using both tissue adhesive and sutures is beyond the scope of this article and the author advises the reader to consult appropriate references as needed.
Uses Beyond Wound Closure
Tissue adhesives have been used for over 100 different “off-label” applications, including skin graft fixation, temporary otoplasty, dental trauma, corneal abrasions, wound sealant, aneurysm embolization, and clitoral avulsion.39-41 Tissue adhesives can also be used to safely repair nail bed lacerations, without magnification, and with only basic surgical training.15 Tissue adhesives appear to be an ideal tool for repairing a split nail plate, no matter how fragmented, and for reaffixing the small pieces of nail for protection of the injured nail bed.15,42,43 When using tissue adhesive for nail bed laceration repair, do not to glue the eponychium to the nail bed because that will interfere with nail growth.
One study found that tissue adhesives excel in the treatment of painful superficial finger fissures caused by the cold temperatures of living in Antarctica.44 Another group also found that tissue adhesive could be used to aid scalp laceration repair using the modified version of the hair apposition technique. In this technique, hair is used to close a laceration by tying knots from opposite sides of the wounds. A single drop of tissue adhesive is used to hold the hair knots together.45 Unfortunately, clinicians can- not bill for a laceration repair using that technique. ■
References
- Penoff Skin closures using cyanoacrylate tissue adhesives. Plastic Surgery Educational Foundation DATA Committee. Device and Technique Assessment. Plastic Recon Surg. 1999;103(2):730-731.
- Watson Use of cyanoacrylate tissue adhesive for closing facial lacerations in children. BMJ. 1989;299(6706):1014.
- Osmond Pediatric wound management: the role of tissue adhesives. Ped Emerg Care. 1999;15(2):137-140.
- Milne CT, Corbett A new option in the treatment of skin tears for the institutional- ized resident: formulated 2-octylcyanoacrylate topical bandage. Geriatric Nursing. 2005;26(5):321-325.
- Gordon Reducing needle-stick injuries with the use of 2-octyl cyanoacrylates for lac- eration repair. J Acad Nurse Pract. 2001;13(1):10-12.
- Singer AJ, Hollander JE, Valentine SM, Turque TW, McCuskey CF, Quinn Prospective, randomized, controlled trial of tissue adhesive (2-octylcyanoacrylate) vs standard wound closure techniques for laceration repair. Stony Brook Octylcyanoacrylate Study Group. Acad Emerg Med. 1998;5(2):94-99.
- Hollander JE, Singer Application of tissue adhesives: rapid attainment of proficiency. Stony Brook Octylcyanoacrylate Study Group. Acad Emerg Med.1998;5(10):1012-1017.
- Quinn J, Maw J, Ramotar K, Wenckebach G, Wells Octylcyanoacrylate tissue adhesive versus suture wound repair in a contaminated wound model. Surgery. 1997;122(1):69-72.
- Wilbur L, Seupaul Evidence-based emergency medicine. Are tissue adhesives an acceptable alternative for simple lacerations? Annals Emerg Med. 2011;58(4):373-374.
- Bruns TB, Worthington Using tissue adhesive for wound repair: a practical guide to dermabond. Am Family Phys. 2000;61(5):1383-1388.
- Singer AJ, Quinn JV, Clark RE, Hollander JE, TraumaSeal Study Closure of lacerations and incisions with octylcyanoacrylate: a multicenter randomized controlled trial. Surgery. 2002;131(3):270-276.
- Quinn J, Wells G, Sutcliffe T, et A randomized trial comparing octylcyanoacrylate tis- sue adhesive and sutures in the management of lacerations. JAMA. 1997;277(19):1527-1530.
- Resch KL, Hick Preliminary experience with 2-octylcyanoacrylate in a pediatric emer- gency department. Ped Emerg Care. 2000;16(5):328-331.