Published on
Urgent message: Industry perception is that urgent care offers the opportunity for potentially substantial cost savings while also providing safe, effective care for complaints of appropriate acuity. Data supporting those claims have been lacking, however.
Lo Fu Tan, MD, MS, FCFP, FAAFP and Jillian Kreston, MBA, MEcon Citation: Tan L F, Kreston J. Cost-effective ambulatory care for emergency department avoidance. J Urgent Care Med. 2022;16(10):25-32.
BACKGROUND
A 2019 brief published by the United Health Group found 18 million “avoidable” emergency room visits that added $32 billion in cost to the healthcare system. Ten common primary care conditions were considered, accounting for 46 million annual ED visits.1 Acute conditions with greater risk of higher acuity and cost of care like shortness of breath were not included. A review of the financial impact of urgent care on ED diversion of low-acuity conditions showed a slight gain in diversion but high and costly utilization.2 Again, high-acuity, more severe conditions were not considered.
Claims for acute, ambulatory care services submitted to United Healthcare (UHC) for its Commercial and Medicaid members and the care delivery organizations for their Medicare Advantage clientele come from many providers, groups, and institutions. In addition to the 275,000 per year seen in the Southwest Medical Associates (SMA) Urgent Care Division, another 375,000 visits occur annually in other urgent care clinics throughout Nevada. However, emergency departments’ submitted claims charges to payers far exceed those of urgent cares.
This study seeks to identify a set of common acute conditions with high acuity and cost to determine if there is an opportunity to save claims charges by having some of these patients traditionally looked after in EDs moved over to urgent care.
METHODS
We reviewed claims submitted for insured members empaneled to Southwest Medical clinicians from 2016 to 2018. Data came from two primary sources: Health Plan of Nevada, a subsidiary of UHC for their commercial and Medicaid members and Southwest Medical, the care delivery organization under OPTUMCare which was at full risk for their Medicare Advantage registrants. A retrospective study was done using propensity score matching. For our control group, we selected ED cases with one of four common acute unscheduled conditions: abdominal pain, chest pain, headache, or shortness of breath using ICD-10 diagnostic codes on claims submissions. Cases were excluded if they were admitted to observation or a hospital from the ED.
We identified patients with the same four conditions who sought care within SMA’s urgent care system for our test group. To reduce the chance of selecting cases that would have been appropriate for the ED or hospital care, we excluded those transferred from urgent care and admitted within 24 hours. To identify initial encounters for these acute conditions, we excluded patients who’d had an ED or urgent care encounter within a month before the index ED visit. These criteria were also applied to the urgent care “treatment” cases.
A propensity score was calculated using a logistic regression or logit model. Given some confounding variables, it is the probability for a patient to belong to one of two groups. Each treatment (urgent care) case was then matched to the closest control (ED) case with similarity evaluated as the distance on the propensity score’s logit function.
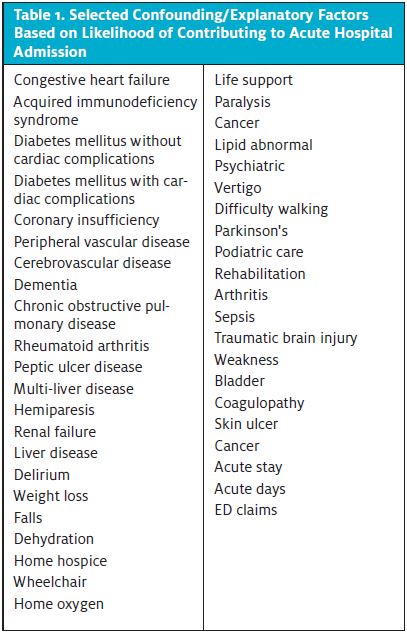
Age and sex were selected as the demographic confounding variables. We excluded race, education, and income only due to unreliable data sources. Other confounding or explanatory factors were selected based on their likelihood of contributing to acute hospital admission. (See Table 1.) Claims records, namely ICD-10 diagnostic codes from the index event, were used.
Cases of other acute conditions were not included due to at least one of these reasons: limited amount and cost of testing or treatment required for these conditions admitted to hospital from ED; transferred from urgent care to ED; or difficulty in matching between ED and urgent care cases.
Average payer claims charge per case was calculated by payer for one of the four acute conditions for the initial visit, the 30 days after, and the two combined. The differences between the ED (control) group and the urgent care (treatment), if any, were determined based on the first condition or test identified by the ICD-10 code search for the index visit.
We followed Austin’s recommendations regarding design, analysis, and reporting for propensity matching:3
- The optimal algorithm in the statistical solution XLSTAT was selected.4
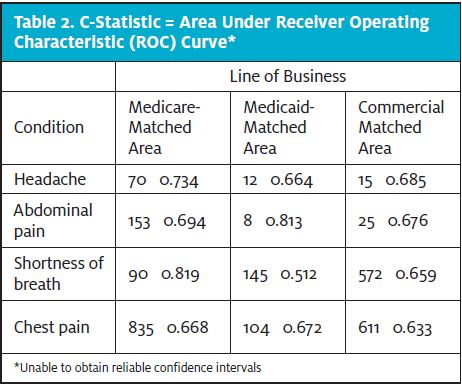
- The balance in baseline characteristics between treated and untreated subjects was compared and reported. To test whether the propensity model had been specified adequately, we used “standardized” differences rather than “hypothesis” testing (ie, receiver operating characteristic curve area [c-statistic].5) C-statistic measures goodness of fit for binary outcomes in a logistic regression model. It equals the area under a receiver operating characteristic curve, ranging from 0.5 to 1.0. If the area is <0.5, then the model is considered poor. If >0.7, it is strong.6
- Finally, appropriate statistical methods for the analysis of matched data were used. We reported Cohen’s d or standardized mean difference (SMD)as the preferred method for estimating treatment effects on outcomes.7
RESULTS
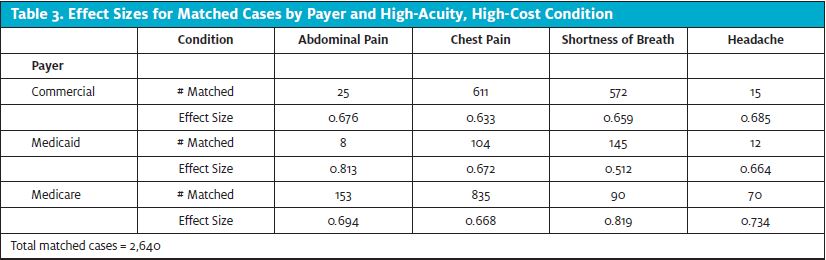
Using traditional research values of p=0.05 for statistical significance and statistical power of 80%, we found that Cohen’s d or SMDfor payer acute condition subgroups were all Moderate (near or above 0.7) when the matched cases exceeded the minimum sample size requirement of 26except in the case of Medicaid shortness of breath, which was Mild (0.5).8 Sample sizes for commercial and Medicaid conditions of abdominal pain and headache were too small to be reliable for any SMD measurement (Table 2). The larger the SMD, the stronger the relationship between the two variables.9 These results indicate that our matching of control ED cases to test urgent care was effective. Table 3 summarizes the number of cases selected for matching using our propensity score method. From 67,975 initial ED visits and 7,798 initial urgent care visits, a total of 2,640 were matched, broken down by payer and by acute condition.
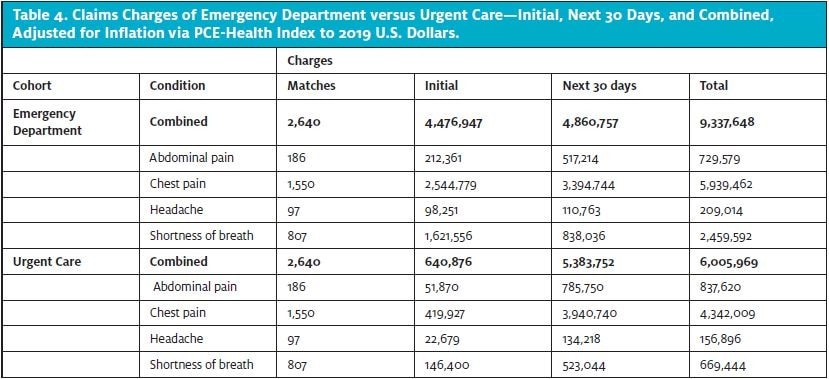
We used the Personal Consumption Expenditure-Health Index to adjust total medical expenditures for inflation over the 3-year study period.10,11 Our study showed total (combined initial visit plus 30-day follow-up period) savings in claims charges of 35% for the propensity score-matched cases when the care was initiated in urgent care ($6.0 million) compared to ED ($9.3 million).
The initial urgent care visit cost of $0.6 million was substantially less than that for the initial ED encounter of $4.5 million, which offset the higher cost over the next 30 days for the urgent care group of $5.4 million vs the ED one at $4.9 million.
By conditions, cost savings occurred for shortness of breath (72% lower when the patient went to the urgent care rather than the ED—$0.7 million vs $2.5 million); chest pain (27%, at $4.3 million vs $5.9 million); and headache (25%, at $159,000 vs $209,000). However, the abdominal pain cohort’s total cost was higher for those seen initially in urgent care by 15%: ($838,000 vs $730,000). See Table 4.
For all payers, the claims charges for any initial visit were less for those seen first in urgent care instead of the ED, no matter the acute condition. However, the same trend did not hold for every payer and condition combination for costs incurred during the 30 days following the initial visit and total combined costs (Table 5).
Commercial matched cases seen in urgent care had a total cost of $1.46 million compared with the ED cost of at $4.65 million. Most of the savings in submitted claims charges occurred with shortness of breath ($1.64 million) and chest pain ($1.56 million). For the 611 commercial chest pain matched pairs, there was a significant difference in total charges between those seen initially in urgent care and those seen initially in the ED ($202,000 compared with $1.77 million, respectively).
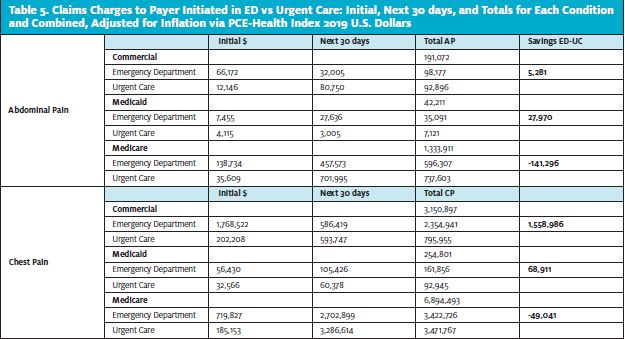
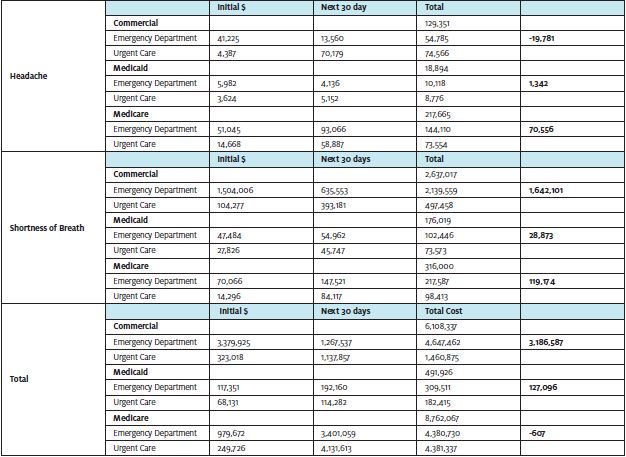
However, over the next 30 days, there was no difference. The shortness of breath group had lower cost in the 30-day follow-up period if seen initially in urgent care, whereas this was higher for both the commercial and abdominal pain and members. There was minimal saving in total claims cost of $53,000 for patients with abdominal pain who presented initially to urgent care. There was a loss of $19,800 within the headache group. However, for commercial abdominal pain and headache, there were not enough matched pairs to determine reliable effect sizes.
For Medicaid, with all four acute conditions, the total cost was lower for members who initially went to the urgent care rather than the ED. The cost saving was $127,000—substantially less than the saving for the commercial group. In part, this was due to the smaller number of matched cases (269 vs 1,223).
Consistent with the commercial finding, chest pain and SOB cases accounted for most of their savings. Thirty-day follow-up costs were lower in all four acute condition groups if first seen in urgent care except for headache, which showed no significant difference. The Medicaid headache group had more cost to the urgent care cases over the next 30 days at $5,200 , but this was only $1,000 more than the matched ED patients. However, the sample size was inadequate. While there was savings over 30 days and total for the abdominal pain group, this sample size was also too small.
Of 1,148 matched Medicare cases, those with headache or SOB had total claims cost savings of $119,000 and $71,000 each, respectively. The chest pain group had a relatively small loss of $49,000, compared with $141,000 for the abdominal pain category. The savings offset these losses in the other two condition groups, leading to overall savings for the Medicare matches.
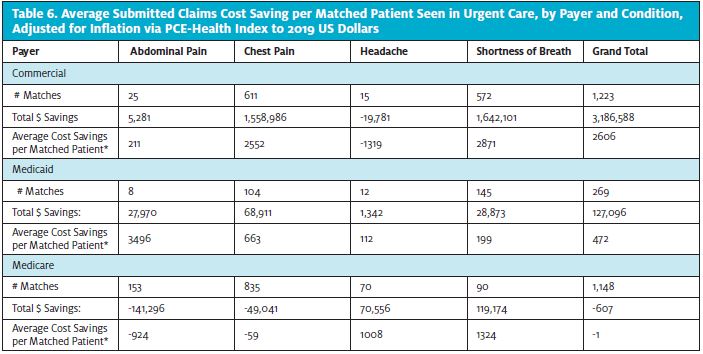
We calculated the average submitted claims cost savings per matched patient seen initially in urgent care (Table 6).
Both SOB and chest pain conditions had considerable savings of over $2,500 per patient of the commercial cases. The cost-saving was small for abdominal pain at $211, and there was a loss for headache of $1,300, but both had inadequate sample sizes. Medicaid chest pain and SOB cases had savings per patient of nearly $700 and $200, respectively. Medicare patients with headache or SOB first seen in urgent care had savings of over $1,000 and $1,300 each. Of note, those with abdominal pain had a loss of nearly $1,000 per case. The chest pain cases had a slight loss of $59 per patient.
DISCUSSION
Overall, an urgent care system capable of providing care for common acute high-acuity conditions requiring more monitoring, testing, and treatment was less costly per matched patient than care provided in EDs. To our knowledge, there has been no previously published evidence of this. The findings supported both payers’ goal of reducing submitted claims charges (HPN with its commercial and Medicaid members and SMA with its Medicare Advantage).
This study focused on membership empaneled to SMA PCPs. While most of our payer membership in the Las Vegas metropolitan area belongs to SMA providers, we do have some non-SMA membership in other Nevada communities. Scaling is dependent on the viability of standing up and maintaining urgent cares that can accommodate cases that otherwise would end up at an ED.
Two limitations that need to be addressed include payer willingness to engage both members and provider groups in redirecting care to these ambulatory settings, and professional and community acceptance.
Why was there a significant difference between chest pain or SOB and abdominal pain or headache? The first two may be better defined and worked up clinically. Due to their inherent life-threatening nature, they often require a more comprehensive workup. The insufficient samples for Medicaid and commercial members with abdominal pain and headache may have played a role. More study is needed, but it may be reasonable to focus on chest pain and SOB for further rationale to establish, maintain, and grow a model of this kind.
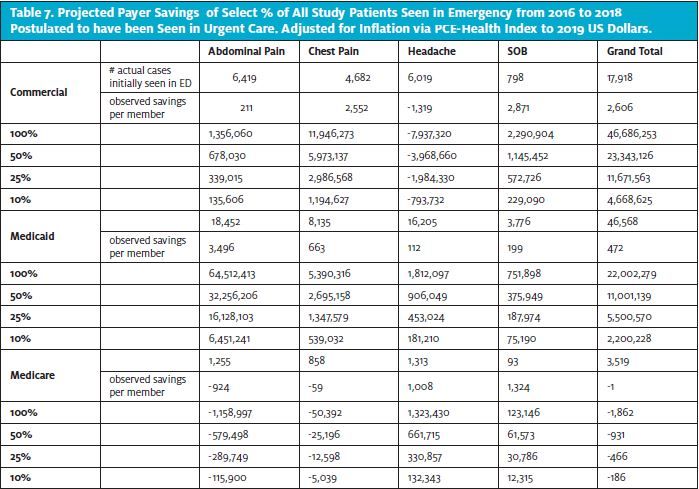
Likely, there would have been more submitted claims charge savings by each high-acuity condition and in combination if we had a larger number of matched cases. Only one third of the total number of 7,780 patients seen initially in urgent care with one of the four conditions was matched during our 3-year study period. Also, over 65,000 study patients seen initially in the ED were not matched to an urgent care case, and we feel that at least some of these could have been seen in urgent care without transfer to the ED. We extrapolated the calculated average savings per matched patient seen first in the urgent care to projected savings for all patients selected who went to the ED from 2016 to 2018. In 100% of the Emergency cases, the potential submitted claims charge savings to all three lines of business (commercial, Medicaid, and Medicare Advantage), and our four selected conditions could have been $69 million. At 50% projected, this would be $38 million saved. Even down to 10%, this is still $6.9 million (Table 7).
It is revealing to look at the breakdown of payer type for these Emergency visits for the four selected conditions. Nearly 30% (28,000) are commercial, 47,000 (70%) are Medicaid, and the remaining 3,500 (5%) Medicare.
The Medicaid group’s high utilization of EDs for these four common acute conditions calls for further study. Our findings suggested value in chest pain and SOB, which might have been confirmed for abdominal pain and headache if the sample size had been enough.
The commercial group, while more minor, is still significant at nearly one third of Emergency visits. The savings from even a small additional number of chest pain and SOB cases diverted to urgent care would be substantial.
Finally, for Medicare, focusing on headaches and SOB may be cost-effective. Simultaneously, considering moving Medicare abdominal pain patients to Emergency from urgent care is worth discussing. The pervading belief is that this population has a relatively high chance of having significant pathology within 3 months of initial presentation with abdominal pain.
We have assumed that all admissions from the ED were necessary. Therefore, these cases were excluded. Counting some could increase the urgent care value proposition.
Consideration should also be given to those patients sent to EDs from urgent cares that are part of the insured network. Most of these clinics can only care for low-acuity conditions like viral URIs, rashes, and UTIs. These urgent care clinics often act as direct conduits for EDs.Southwest Medical has a protocol that requires non-emergent patients to get prior authorization from a medical director before being sent to an ED for evaluation.
LIMITATIONS
The study has limitations. First, we analyzed only patients with one of four acute high-acuity conditions. Others have limited testing, monitoring, and treatment needs, making ED evaluation less warranted. Ideally, we would determine precisely what is causing any difference in costs—for example, in ED procedures or tests vs higher ED charges or both.
We only used one propensity score measure, albeit a reliable one for this purpose.12 As some feel that matching is not an appropriate method since it can accomplish the opposite of its intended goal of preprocessing data for causal inference,13 we should do the study using other propensity score tests. Propensity matching cannot control for unobserved differences associated with treatment (using UC) and outcome (cost), which means that it is essential to consider whether or not covariates used in the propensity model are adequate (ie, is there unobserved acuity/severity in these ED patients that are not being captured?). We excluded those who were admitted to the hospital to limit this.
A prospective study would be ideal, but this may not be practical due to cost and ethical considerations. A time-series analysis of changes in the total acute care spending UC vs ED instead of limited to four conditions would be a reasonable next step.
We did not look at costs other than to the payer as submitted claims charges for the initial and follow-up period of 1 month of care. Urgent cares’ investment and maintenance spending to support high-acuity cases should be reviewed in a future cost-benefit analysis. While we would like to know the actual difference in costs for treating similar conditions at the ED vs the UC, this is challenging due to the considerable heterogeneity in patients who use EDs over UCs.
Finally, data regarding UC/ED utilization pattern change over time with more UCs would be welcomed.
CONCLUSION
In conclusion, instead of an ED, using an urgent care capable of looking after selected higher-acuity cases led to submitted claims charge savings for the payers, HPN (commercial and Medicaid members), and SMA (Medicare Advantage members). More study needs to be conducted, but there is an opportunity to increase savings using this model. Scaling this ought to be explored.
REFERENCES
- United Health Group. Health Brief: 18 million Avoidable emergency department Visits Add $32 Billion in Costs to the Health Care System Each Year. United Health Group; 2019.
- Hall JA, Summers KH, Obenchain, RL. Cost and utilization among propensity score-matched insulin lispro and regular insulin users. J Manag Care Pharm. 2003;9(3):263-268.
- Manca A, Austin PC. Using propensity score methods to analyze individual patient‐level cost‐effectiveness data from observational studies. HEDG Working Paper 08/20, the University of York; 2008.
- XLSTAT version 2020.2. Paris: Addinsoft Inc. (https://www.xlstat.com/fr/ January 30, 2020).
- Austin PC. Report card on propensity-score matching in the cardiology literature from 2004 to 2006. A systematic review. Circ Cardiovasc Qual Outcomes. 2008;1(1):62-67.
- C-Statistic: Definition, Examples, Weighting, and Significance. Practically Cheating Statistics Handbook. WordPress; 2016.
- Hosmer DW, Lemeshow S. Applied Logistic Regression (2nd ed). New York, NY: John Wiley & Sons; 2000.
- McGough JJ, Faraone SV. Estimating the size of treatment effects. Psychiatry (Edgmont). 2009;6(10):21-29.
- Imbens GW, Rubin DB. Causal Inference for Statistical, Social, and Biomedical Sciences. An Introduction. New York, NY: Cambridge University Press; 2015.
- Dunn A, Gross SD, Zuvekas SH. Adjusting health expenditures for inflation: a review of measures for health services research in the United States. Health Serv Res 2018;53(1):175-196.
- AHRQ. 2020. Using appropriate price indices for analyses of health care expenditures or income across multiple years. Available at: https://meps.ahrq.gov/about_meps/Price_Index.shtml. Accessed June 8, 2022.
- Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399-424.
- King G, Nielsen R. Why propensity scores should not be used for matching. Political Anal. 2019;27(4):1-20.
Author affiliations: Lo Fu Tan, MD, MS, FCFPC, FAAFP is Sr. Medical Director, Digital Health, OPTUMCare. Jillian Kreston, MBA, MEcon is Risk and Quality Director, Health Economics, OPTUMCare.
Read More
- Reducing Low-Acuity Preventable Emergency Room Visits By Utilizing Urgent Care Center Services Via Mobile Health Unit Diversion Program
- Urgent Care Centers Can Reduce ED Referrals For CT Scans In Mild Head Injury With Integration Of Brain Activity Biomarker
- The Effect Of PECARN Guidelines On Minor Head Injury Referrals From The Urgent Care Center To The Emergency Room