Published on
Urgent Message: Boxer’s fractures are among the most common hand fractures and should be suspected in cases of closed fist injury. Additionally, a laceration that accompanies a boxer’s fracture may represent a fight bite, which should be treated to reduce the risk of infection.
Jennifer Hicks, DO; Bradley Strauch, MD
Citation: Hicks J, Strauch WB. Urgent Care Evaluation and Management of Boxer’s Fractures. J Urgent Care Med. 2024; 18(8):32-36
Editor’s Note: While the images presented here are authentic, the patient case scenarios are hypothetical.
Clinical Scenario
An 18-year-old male presents with pain in the ulnar aspect of his right hand after he punched a wall 2 hours earlier. He has increased pain with motion, a minimal amount of numbness in the pinky finger, and notes immediate swelling over his knuckles. He denies pain in the wrist and elbow or any other acute complaints.
On exam, he is minimally tachycardic, but his vitals are otherwise normal. He isalert and in no distress, holding his hand in his lap.There is obvious swelling to the dorsal and ulnar aspects of the hand and moderate tenderness to palpation over the metacarpal phalangeal (MCP) joint of the little/pinky finger. There is increased pain with active hand movements, and his range of motion is significantly reduced at the MCP joint of the little finger. There is no tenderness over the proximal interphalangeal (PIP) or distal interphalangeal (DIP) joints of the little finger or over the MCP of the ring finger. The proximal hand, wrist, and elbow are non-tender with normal range of motion. Distal capillary refill of all fingers is brisk, and the patient has sensation to all fingers.
An x-ray of the right hand is obtained, demonstrating a fracture of the 5th metacarpal neck with approximate 30 degrees of angulation deformity (Image 1).
Relevant Anatomy
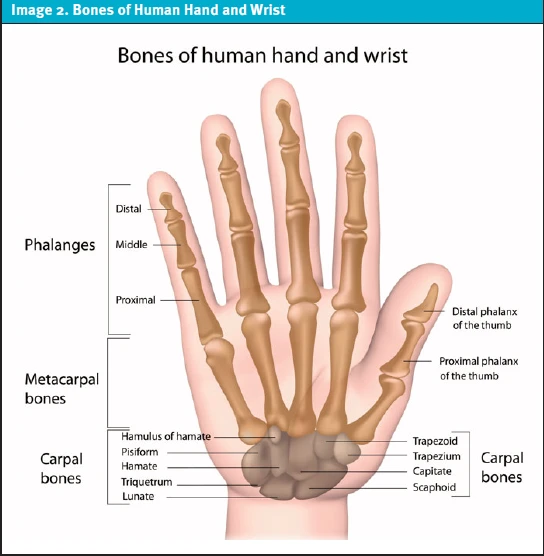
The index, middle, ring, and little fingers each have 3 phalanges: the proximal, middle, and distal phalanx (Image 2).
Boxer’s Fracture
A “boxer’s fracture” is one of the most common hand injuries. It most often occurs in younger patients who strike a hard surface—such as a wall or another’s face—with a closed fist. A boxer’s fracture is a fracture of the 5th metacarpal neck (little finger). The degree of angulation is measured on the oblique and/or lateral view, which determines if reduction is necessary.[1] Another sign that reduction should be performed is pseudo-clawing. Pseudo-clawing is hyperextension of the MCP and flexion of the PIP with attempted extension of the injured hand.1 A carpal-metacarpal (CMC) dislocation can also occur with more forceful mechanisms.
Any closed fist injury (CFI) that results in a fracture with a laceration should be treated as an open fracture, which will significantly affect management and can result in serious infectious complications.[2]
History
The most typical mechanism of injury involves a CFI where the 5th MCP (little finger) strikes the hard surface. It is important to assess whether there was a possibility of CFI to the mouth (ie, a “fight bite”) as the risk of forceful contamination with oral flora dramatically increases risk for infection. Infections can range from superficial skin infection to something more serious, such as tenosynovitis or a septic joint. Infection occurs in a significant percentage of closed fist injuries. Additionally, “fight bites” raise concern for the possibility of retained tooth fragments or other macroscopic debris that may further increase infection risk. Consider imaging if this is a consideration.[3]
The pain associated with boxer’s fractures is usually most significant at the fracture site near the 5th MCP joint. Pain is exacerbated with movement, and range of motion is usually reduced. Associated symptoms may include swelling, paresthesias, and bleeding. Pain present at the proximal joints (ie, wrist and elbow) or distal joints (ie, PIP, DIP) should be explored further to determine if additional radiography exams would be required.
Physical Examination
Exam should focus on evaluation of swelling, areas of tenderness, and most importantly, defects in the skin. Palpating the area of greatest pain as well as the extremity to the joint proximal and distal to the injury (ie, distal finger to the elbow) is helpful for excluding other associated injuries. It is important to assess range of motion, flexor and extensor tendon function, and neurovascular status by documenting sensation, capillary refill, and pulses.
Rotational deformity can be assessed by having the patient flex their digits onto the palm. Extending a line out from each of the fingers, the lines should converge near the scaphoid navicular.[4] Convergence of these lines indicates normal rotation, while divergence of the little finger indicates rotational dysfunction. Another way to assess this is to have the patient flex the MCP to 90 degrees while extending the PIP and DIP. If rotational alignment is normal, the fingers should be in a straight line in this position. It is helpful to compare any rotation to the opposite hand as some individuals have some natural rotation of the little finger.[5]
Radiography
A stepwise approach to evaluation of a hand x-ray (XR) will avoid missing important findings. Assess the metacarpal bones looking for alignment, signs of soft tissue swelling (indicating location of greatest injury), and fracture. Fractures will appear as a break in the cortex on any of the 3 views, disruption in trabeculations, lucency within the bone, and/or angulation or impaction. Evaluate the bones of the wrist (carpal bones) for fractures—specifically looking at the hamate bone with a boxer’s fracture—or dislocation. Obtain a dedicated wrist x-ray if wrist palpation or range of motion elicit pain.
“Evaluate the bones of the wrist (carpal bones) for fractures— specifically looking at the hamate bone with a boxer’s fracture — or dislocation.”
Management
First, it must be determined if reduction is necessary. If there is 30-50 degrees or less of angulation of the 5th metacarpal, this is acceptable, and the injury does not require reduction for a functional outcome.[6] With higher degrees of angulation, reduction can be offered to help minimize the resultant cosmetic deformity.[7] If there is significant angulation, sometimes a modified lateral view can be obtained to help make a decision regarding reduction. Note that a rotational deformity will often not be corrected with closed reduction. If there is no need for reduction, splinting with an ulnar gutter splint to the immobilize the joint proximal and the joint distal to the injury is usually appropriate.
In recent years, increasing evidence has immerged suggesting functional wrapping or buddy taping may be acceptable alternatives to rigid splint immobilization.[8],[9] However, as this has yet to meet universal acceptance, it is prudent to continue fully immobilizing the fracture as described above unless real-time consultation with the hand specialist is possible. Caution the patient that some degree of cosmetic deformity can occur. After splinting, discuss splint maintenance, analgesia, and the role of ice and elevation. Patients should be referred to an orthopedist or hand surgeon as soon as possible, but ideally within 1 week.
Closed reduction has fallen out of favor in the last decade in favor of surgical repair when indicated. Surgical repair is increasingly reserved for open or intraarticular fractures or cases where significant functional impairment is expected.[10]
A fracture resulting from a CFI involving a mouth requires special treatment as oral organisms may be introduced resulting in septic arthritis, tenosynovitis, or osteomyelitis. These CFI, colloquially referred to as “fight bites,” have disproportionately higher associated morbidity compared with other CFI. Additionally, patients may be reluctant to reveal the etiology of the injury for fear of legal or other social issues. Fight bites often present with a laceration over the MCP joint of the middle, ring finger, or little finger. Subsequent infection can track along the subfascial and subcutaneous spaces on the dorsum of the hand.[11] Joint penetration occurs in over 90% of cases, and septic arthritis occurs in 12% of cases.[12] The incidence of osteomyelitis and tenosynovitis are reported to be 15-25%.[13] Fight bite infections are usually polymicrobial. Talan et al showed that the median number of isolates per wound culture was 4, with common organisms being streptococcus, staphylococcus, eikenella corrodens, and fusobacterium.[14]
Patients with a boxer’s fracture (or any other hand fracture) and with an overlying fight bite should be treated as having an open fracture and therefore immediately referred to a local emergency department (ED) with orthopedics coverage for possible surgical debridement and intravenous antibiotics. Instruct patients not to eat or drink before referring them as there is a high probability urgent intervention in the operating room may be recommended. For patients with fight bites without associated fracture, aggressive wound care with copious irrigation in urgent care (UC) is critical. The recommended first-line antibiotic after fight bite injuries is amoxicillin/clavulanate. In patients with true penicillin allergy, doxycycline, ciprofloxacin, or trimethoprim/sulfamethoxizole in combination with metronidazole or clindamycin is recommended.[15] In addition to antibiotic prophylaxis, ensure that the patient’s tetanus vaccination status is up-to-date.
Next-Level Urgent Care Pearls
- Experienced providers can accomplish closed reduction of boxer’s fractures in urgent care. If provider training and comfort allows, consider utilizing a hematoma block to allow for better patient comfort when apply pressure and traction. Ensure the neurovascular status of the hand is intact before and after the procedure. Obtain post-reduction x-rays to evaluate for the quality of the reduction. Place the hand in an ulnar gutter splint and refer the patient for follow-up with orthopedics or hand surgery as described above after confirming improved alignment.8 For injuries not requiring reduction, ulnar gutter splints remain the most prudent initial immobilization measure. However, there is growing controversy about this (as stated above) with some recent studies showing non-rigid splint or buddy taping for initial immobilization resulting in comparable outcomes.8,9
- Exploration for other mechanisms of injury or social concerns include:
- Fight bite – Specifically ask if the injury occurred by contact with teeth. This will change management and require antibiotic prophylaxis.
- Domestic abuse – If a patient situation is concerning for intimate partner violence, inquire about the safety of the patient’s living situation and offer community resources for domestic abuse support/counseling.
- Altercation – If the injury occurred because of an altercation, consider other injuries the patient may be unwilling to report, including head or neck injury.
- Remember to ensure the patient history makes sense. Many patients with CFI may not be forthcoming about the circumstances of the injury due to the sensitive nature of certain injuries, including:
- Injuries from child or domestic abuse
- Injuries from alternative sexual practices
- Illegal drug use or interpersonal violence
- Nonconsensual sexual relations
- Injuries with potential legal ramifications
Clinical Scenario Conclusion
An XR showed a fracture of the 5th metacarpal neck, consistent with a boxer’s fracture. There was 30 degrees of angulation, not requiring a reduction. The patient was splinted in an ulnar gutter fiberglass splint and asked to follow up with orthopedics within 3-5 days. The patient followed up as instructed, and the splint was changed to a cast. The patient was immobilized for 4 weeks, and the cast was removed with a good functional outcome.
Takeaway Points
- Boxer’s fractures are among the most common hand fractures and should be suspected in cases of closed fist injury.
- If the angulation of the 5th metacarpal neck is 30-50 degrees or less, reduction is not necessary.
- Specifically evaluate for the rare, but serious possibility of a carpal-metacarpal dislocation.
- A laceration which accompanies a boxer’s fracture may represent a fight bite and should be treated as an open fracture. These injuries warrant immediate evaluation in an ED with orthopedics specialty coverage.
- CFI without associated fracture can be irrigated extensively and treated with oral outpatient antibiotics, but ensure close follow-up and strict ED precautions given the high rates of serious associated infection.
- Surgical repair of 5th metacarpal fractures is controversial and is becoming increasingly reserved for more complicated fractures. However, given that boxer’s fractures are usually dominant hand injuries, orthopedics follow-up as soon as possible, ideally within 1 week, is prudent to ensure that alignment is appropriate, and closed reduction is not indicated.
Manuscript submitted February 6, 2024; accepted April 4, 2024.
Author Affiliations: Jennifer Hicks, DO, PGY-1, Adena Health System. W. Bradley Strauch, MD, Adena Orthopedic and Spine Institute, Chillicothe, Ohio. Authors have no relevant financial relationships with any ineligible companies.
References
- [1]. Diaz-Garcia R, Waljee JF. Current management of metacarpal fractures. Hand Clin. 2013;29(4):507-518. doi:10.1016/j.hcl.2013.09.004
- [2]. Kennedy SA, Stoll LE, Lauder AS. Human and other mammalian bite injuries of the hand: evaluation and management. J Am Acad Orthop Surg. 2015;23(1):47-57.
- [3]. Soong M, Got C, Katarincic J. Ring and little finger metacarpal fractures: mechanisms, locations, and radiographic parameters. J Hand Surg Am. 2010;35(8):1256-1259. doi:10.1016/j.jhsa.2010.05.013
- [4]. Burkhalter WE. Closed treatment of hand fractures. J Hand Surg. 1989;14(2 Pt 2):390-393. doi:10.1016/03635023(89)90120-2
- [5]. Henry MH. Fractures and dislocations of the hand. In: Rockwood and Green’s fractures in adults, 6th edition, Bucholz RW, Heckman JD, Court-Brown C (Eds), Lippincott, Williams & Wilkins, Philadelphia 2006. p.772.
- [6]. Diaz-Garcia R, Waljee JF. Current management of metacarpal fractures. Hand Clin. 2013;29(4):507-518. doi:10.1016/j.hcl.2013.09.004
- [7]. Strub B, Schindele S, Sonderegger J, Sproedt J, von Campe A, Gruenert JG. Intramedullary splinting or conservative treatment for displaced fractures of the little finger metacarpal neck? A prospective study. J Hand Surg Eur Vol. 2010;35(9):725-729. doi:10.1177/1753193410377845
- [8]. Van Aaken J, Kämpfen S, Berli M, Fritschy D, Della Santa D, Fusetti C. Outcome of boxer’s fractures treated by a soft wrap and buddy taping: a prospective study. Hand (N Y). 2007 Dec;2(4):212-7. doi: 10.1007/s11552-007-9054-2. Epub 2007 Jul 3. PMID: 18780055; PMCID: PMC2527222.
- [9]. Mohamed MB, Paulsingh CN, Ahmed TH, Mohammed Z, Singh T, Elhaj MS, Mohamed N, Khan S. A Systematic Review and Meta-Analysis of the Efficacy of Buddy Taping Versus Reduction and Casting for Non-operative Management of Closed Fifth Metacarpal Neck Fractures. Cureus. 2022 Aug 26;14(8):e28437. doi: 10.7759/cureus.28437. PMID: 36176848; PMCID: PMC9512295.
- [10]. Hussain MH, Ghaffar A, Choudry Q, Iqbal Z, Khan MN. Management of Fifth Metacarpal Neck Fracture (Boxer’s Fracture): A Literature Review. Cureus. 2020;12(7):e9442. Published 2020 Jul 28. doi:10.7759/cureus.9442)
- [11]. Smith HR, Hartman H, Loveridge J, Gunnarsson R. Predicting serious complications and high cost of treatment of tooth-knuckle injuries: a systematic literature review. Eur J Trauma Emerg Surg. 2016;42(6):701-710. doi:10.1007/s00068-016-0701-6
- [12]. Shewring DJ, Trickett RW, Subramanian KN, Hnyda R. The management of clenched fist ‘fight bite’ injuries of the hand. J Hand Surg Eur Vol. 2015;40(8):819-824. doi:10.1177/1753193415576249
- [13]. Eilbert WP. Dog, cat, and human bites: providing safe and cost-effective treatment in the ED. Emerg Med Prac 2003;5:1-20
- [14]. Talan DA, Abrahamian FM, Moran GJ, et al. Clinical presentation and bacteriologic analysis of infected human bites in patients presenting to emergency departments. Clin Infect Dis 2003 Dec 1; 37(11):1481-1489
- [15]. Stevens DL, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America. Clin Infect Dis. 2014;59(2):147.
Download the article PDF: Urgent Care Evaluation and Management of Boxer’s Fractures
Read More