Published on
Urgent message: Timely employment—and informed selection—of the most suitable mode of imaging are essential for correct diagnosis and optimal treatment of scaphoid injuries in the urgent care setting, often negating the need for referral to a higher-acuity setting.
Muhammad Asim, MBBS, FRNZCUC, FRNZCGP and Rabeeah Asim, MBBS
INTRODUCTION
The scaphoid is the most commonly injured bone amongst carpal bones at the wrist, accounting for 10% of all hand fractures and 50% to 80% of all carpal fractures. Risk of nonunion is up to 10% in all nondisplaced fractures.1 This injury is frequent in adults and athletes who fell on their outstretched hand. There are serious consequences with misdiagnosis or delayed diagnosis such as non-union, avascular necrosis, and arthritis. A high index of suspicion based on the mechanism of injury, clinical exam, followed by immobilization with delayed x-rays can prevent these complications.
Early MRI for suspected scaphoid injuries found scaphoid fracture in 40% of x-ray negative patients.2 Early referral to a specialist orthopedic or plastic surgeon for displaced fractures or if there is evidence of nonunion on follow-up can help prevent long-term complications and disability.3
CURRENT PRACTICE IN URGENT CARE
Current practice for suspected scaphoid fracture with a negative x-ray in many urgent care clinics is to immobilize using a scaphoid cast and have the patient follow up in 10-14 days with repeat x-ray to look for evidence of fracture or callous formation. For confirmed fractures with no displacement, the period of immobilization is based on the fracture site (distal, mid, or proximal pole). Displaced fractures or open injuries are referred acutely to orthopedics.
CASE DESCRIPTION
CA is a 20-year-old male, right-hand dominant barista who presented to the urgent care clinic on December 5. He sustained an injury the previous day after falling backwards onto his left outstretched hand (FOOSH). Initially he thought it was a sprain, but movements were causing a lot of pain, so he presented to urgent care. There were no other injuries and no pain in the elbow or shoulder area. He was wearing a splint he happened to have at home. There was no significant past medical history. He was not known to have any drug allergies.
Meds
Acetaminophen and ibuprofen PRN for pain.
Family History
Father had osteoarthritis of the hip needing joint replacement in his 60s.
Personal History
Smoker, 3-4 per day.
On Examination
Alert, mildly distressed due to pain. OBS stable Afebrile.
Left wrist: Closed injury with no obvious swelling or deformity.
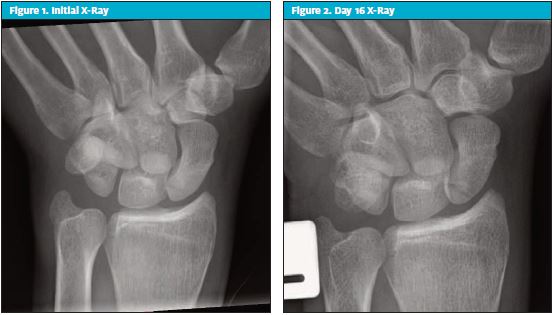
There was tenderness to the radial aspect of the wrist and at the anatomical snuff box (ASB) area. He had painful movements at the wrist and to the base of thumb. There was also central dorsal and volar tenderness of the wrist. The triangular fibrocartilage complex grind test was negative. Elbow and hand examination was normal with no neurovascular deficit to the hand. X-ray of the left hand and wrist was suspicious for a proximal pole fracture (see Figure 1).
Impression
Nondisplaced left scaphoid fracture.
Plan
The patient was placed in a scaphoid cast (below elbow back slab with thumb spica) and arm sling for elevation. He was scheduled for 2-week follow-up in the same urgent care center. Analgesia was prescribed and he was advised to avoid use of NSAIDs.
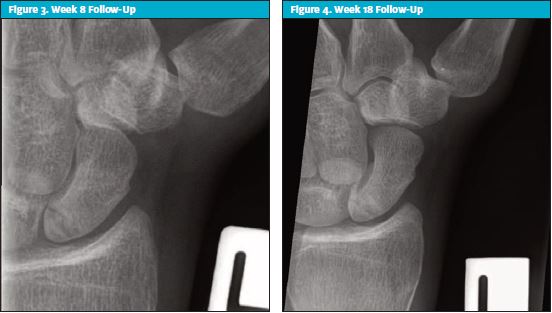
Day 16 Post Fracture
Repeat x-rays did not show any change. The patient still had slight tenderness to the ASB area and tenderness to axial loading. He was placed in a below elbow fiber glass (BEFG) scaphoid cast with a waterproof liner (on patient request). See Figure 2.
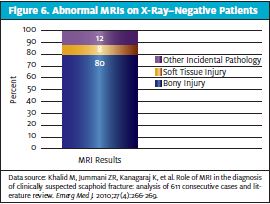
Week 8 Follow-Up
Nontender at snuffbox and scaphoid tubercle in left hand. Wrist movements were normal with mild out-of-cast stiffness and weakness. X-ray of left scaphoid was reported as showing early healing or bone bridging. Patient was removed from BEFG cast and fitted with a scaphoid splint. He was referred to hand physiotherapist and with advice for light activities only. See Figure 3.

Week 18 Follow-Up
Ongoing pain at scaphoid area while doing movements out of splint. Repeat x-ray was showed minor sclerosis at bony ends, features consistent with non-union; advised CT scan. Patient was referred to orthopedic surgeon for CT scan. See Figure 4.
Week 21 Follow-Up
Patient had full range of movements with slight discomfort and was referred for a CT- scan. CT-scan showed some sclerosis across the fracture line consistent with new bone formation. (See Figure 5.) Patient is awaiting review by orthopedic surgeon following CT scan.
DISCUSSION
Incidence
The scaphoid is the most commonly fractured wrist bone, with injury usually occurring following a fall on an out-stretched hand (FOOSH). Injury to the scaphoid is difficult to diagnose and immobilization of the wrist based on clinical impression is common. Scaphoid fracture accounts for 10% of all hand and up to 70% of all carpal bone fractures, making it the most common injury of carpal bones at the wrist.1,3 Wolf, et al reported that the peak incidence of scaphoid fracture is in 20- to 24-year-olds and is more common in male gender.2
Anatomy
The scaphoid bone has an irregular shape and up to 80% of the bone is covered by articular cartilage. The blood supply to the scaphoid bone has been well described by Panagis, et al, who showed that dorsal vessels supply 80% of the vascularity to the scaphoid and the majority of blood enters via dorsal ridge. Due to the unique vascularity, proximal pole fractures have a worse prognosis for healing than distal injuries.5 Fractures to the scaphoid bone are classified by location: distal pole, waist, and proximal pole. The majority occurs at the waist (65%), followed by proximal pole (15%), and then distal body (10%); 8% occur at the tuberosity.6
Mechanism of Injury
The most common mechanism of scaphoid fracture is a FOOSH common to many sporting injuries. With FOOSH, direct vertical compression force goes along the long axis of the wrist with hyperextension to more than 95° and causes the central scaphoid body to be forced against the dorsal end of the distal radius, causing its fracture. A direct blow or a twisting injury is unlikely to cause fracture of the scaphoid.7
Diagnosis
The most important tool to diagnose or suspect scaphoid fracture (after mechanism of injury) is clinical examination. Tenderness in the anatomical snuffbox (ASB) is a widely used and known test to diagnose scaphoid fracture. This test is very sensitive but has specificity of only 40%. It can be falsely positive if the radial nerve sensory branch is pressed in the ASB.8 Pain on longitudinal compression of thumb is 100% sensitive but has specificity of only 30% while localized tenderness to the scaphoid tubercle has a specificity of 48%.9 Combining all the tests can give a good indication of scaphoid injury during initial evaluation.
There is controversy in regard to sensitivity and specificity of history and physical signs for diagnosis of scaphoid fractures. Carpenter, et al did a systematic review of 75 studies for diagnosis of scaphoid fracture in ED and acute settings. The authors concluded that, in the absence of tenderness to the scaphoid and pain on resisted supination of forearm, there is a low likelihood of having scaphoid fracture with negative likelihood ratios of 0.15 and 0.09, respectively. History was also not a significant or useful tool for diagnosis of scaphoid fracture.10
Imaging
Plain radiograph of the wrist, including a scaphoid view, is the initial investigation but can miss around 20% of fractures; the most frequently missed area is the middle portion of the scaphoid bone. Scapholunate disruption is another important injury to identify on plain radiograph. Plain radiographs are also poor at showing displacement of fracture fragments. Bernard, et al reported sensitivity of 78% and specificity of 72% to detect 1 mm displacement by plain radiograph.11 If there are any doubts about displacement of fracture segments, the patient should be referred for CT via orthopedics acutely in hospital. Mallee, et al reported that plain radiographs are limited in their ability to detect the scaphoid fracture within 2-6 weeks, especially oblique fractures of the middle third of the scaphoid body, which if missed can lead to poor outcome and complications.12 Consequently, follow-up at 2 weeks with repeat imaging is recommended.
CT scan has sensitivity of 72% and specificity of 99% to detect scaphoid fractures, including displacement of fracture segments, but can`t detect most soft tissue injuries. Timing after injury has no effect on the accuracy of CT scan. Simply speaking, it would miss 56 fractures in 1,000 patients and overtreat eight patients.10
MRI scan has sensitivity of 88% and specificity of 100% to detect scaphoid fractures and can also detect soft tissue injuries. It is the best test to do for suspected scaphoid fractures. MRI is the most accurate imaging test to confirm scaphoid fracture in ED patients and if it is not available acutely then CT scan is next imaging modality to rule out fracture.10
Bone scan has the highest sensitivity (99%) to detect scaphoid fractures but lacks specificity ( 86%) and it is best done 72 hours after injury, so it is not the investigation of choice for the scaphoid fracture.10
There is no consensus in the literature about the best imaging modality to diagnose scaphoid fracture, and no one is identified as the gold standard. Mallee, et al concluded from systematic review of different studies that two such standards may be reasonable: positive plain radiographs at 6 or more weeks post injury or agreement of at least two advance modalities—MRI, CT, or bone scan.12
Management
Initial treatment of suspected scaphoid fracture is by-case immobilization. Immobilization should be considered even with negative radiographs. If x-rays are negative, then advanced imaging can be performed based on patient preferences, cost, and availability. High-end athletes and professionals who can’t afford unnecessary immobilization should be referred early to Orthopedics for consideration of CT or MRI, or should be given option to self-pay for the scan. Initial follow-up should be in 2 weeks, with repeat x-ray.3
Red Flags for Specialist Referral
Indications for referral to a specialist include open fracture with or without neurovascular compromise (acute), proximal pole fractures (within weeks to specialist), fracture segment displacement of more than 1 mm, delayed presentation (more than 3 weeks), scapholunate rupture (more than 3 mm widening) and routine referral if there is evidence of nonunion on follow-up visits while patient is being managed conservatively.13
For casting of scaphoid fracture, controversy exists regarding whether the thumb should be included. Leaving the thumb out gives the patient more freedom. Buijze, et al compared both in multicenter randomized controlled trials for casting of scaphoid fracture with or without thumb immobilization. There were higher rates of fracture union confirmed by CT at 10 weeks in the group treated without thumb immobilization. Functional and pain outcome and radiological union rates at 6 months were the same in both groups. This trial didn’t include large numbers and the study lacks power.14 A thumb-free cast is an option for people wanting more mobility of the thumb for their profession while being managed conservatively. In our center we put patients on standard below elbow thumb spica scaphoid cast.
Period of immobilization for fracture healing depends on the location of the fracture due to the unique blood supply of the scaphoid bone. Distal pole fractures need an average of 6 weeks in cast while mid-pole fractures need 12 weeks of immobilization. Proximal pole fractures may require up to 20 weeks of immobilization in cast.3,6 In the case described here, the decision to go for 12 weeks of immobilization may be held by some to be overly conservative. Another option would have been to refer early to orthopedics for consideration of surgery.
Surgery for scaphoid fractures can shorten the healing time and can expedite the return to sports or work for patients. Inoue, et al reported equal healing rates in both surgical and nonsurgical groups with mid-body fractures but time to return to sports was 5.8 weeks in the surgical group compared with 10.2 in the nonsurgical group.15 Patients who have evidence of nonunion, especially patients with proximal pole fractures, need surgery with internal fixation and bone grafting. The bone graft is usually taken from the iliac crest but more recently the distal radius is also being used.16 Surgery is the best treatment for proximal pole and mid-pole fractures, which should also be referred early to an orthopedic or hand surgeon. Surgery can help patients recover quicker and can prevent long-term complications. It is necessary to balance risk and benefits, however, as surgery is not without risks.
Complications of Scaphoid Fracture
- Avascular necrosis – Proximal 1/3 of fractures
- Nonunion of fracture fragments – Main factor being delayed or inadequate immobilization and also site of fracture due to unique blood supply to scaphoid bone.
- Chronic pain and arthritis – Steroid injection can help with arthritis and chronic pain and surgery with arthrodesis is an option if steroid injection doesn’t work.17
In summary, scaphoid fracture management is an important subject that every urgent care, sports medicine, and emergency medicine physician should be prepared to deal with. It is important for urgent care physicians to be aware when to refer these patients for surgery or specialist opinion. (In New Zealand, advanced imaging utility is restricted to specialists only in due to cost restraints imposed by the country’s Accident Compensation Corporation [ACC, a government insurance program], which may delay adequate care for some patients.) Scaphoid injury, if missed or poorly managed, can have long-term consequences for patients, especially athletes.
In this particular case, this patient should have been given the option of an early surgical opinion regarding surgery compared with conservative management of 16-20 weeks in cast immobilization. If conservative treatment had failed, the patient could always go for the surgical option with bone grafting (though recovery time and return to sports or full duties at work might have delayed). Ideally, the patient would undergo MRI scan of the scaphoid if initial x-ray is negative or there is uncertainty about displacement of fracture fragment. MRI is more expensive than CT but is the best modality to diagnose the scaphoid fracture and the soft tissue injury at same time. Its use can prevent unnecessary immobilization and the time off from work.
Achieving Optimal Results
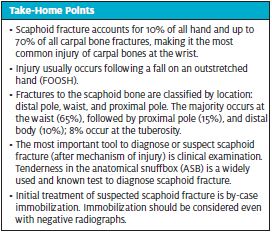
Early MRI can help exclude scaphoid fracture. Canberra Area Scaphoid Trial 200518 included patients who had an initial normal x-ray of the scaphoid with clinical suspicion of fracture. MRI was highly sensitive and specific to rule out scaphoid fracture. They concluded that early MRI is a sensitive and practical way to diagnose occult scaphoid fracture and that it can help avoid unnecessary cast immobilization for these patients. This was a small study and lacks power. However, a larger study including 611 patients by Khalid, et al, had similar findings.19 Abnormal MRIs on x-ray-negative patients showed bony injury in 80%, soft tissue injury in 8%, and other incidental pathology in 12%.
Patient anxiety and time off from work can be minimized with use of advanced imaging in acute care. Cost is the main concern in doing MRI in acute settings. A study by Patel, et al that compared cost and patient satisfaction showed that the MRI group had better pain and satisfaction scores with comparable time off work and sporting activities. Early MRI was marginally cost-effective compared with the conventional treatment group.20
CONCLUSION
Early specialized images in form of MRI can diagnose scaphoid fracture and guide specific treatment at urgent care clinics.
REFERENCES
- Alshryda S, Shah A, Odak S, et al. Acute fractures of the scaphoid bone: systematic review and meta-analysis. Surgeon. 2012;10(4):218-229.
- Brydie A, Raby N. Early MRI in the management of clinical scaphoid fracture. Br J Radiol. 2003;76(905):296-300.
- Eiff MP, Hatch RL, Calbach WL. Carpal fractures. In: Eiff MP, Hatch RL, eds. Fracture Management for Primary Care. 3rd ed. Philadelphia, PA; Saunders: Philadelphia.
- Wolf JM, Dawson L, Mountcastle SB, Owens BD. The incidence of scaphoid fracture in a military population. Injury. 2009;40(12):1316-1319.
- Panagis JS, Gelberman RH, Taleisnik J, et al. The arterial anatomy of the human carpus. Part II: the intraosseous vascularity. J Hand Surg. 1983;8(4):367-375.
- Seitz WH Jr, Papandrea RF. Fractures and dislocations of the wrist. In: Bucholz RW, Heckman JD, eds. Rockwood and Green’s Fractures in Adults. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002.
- Dobyns JH, Beckerbaugh RD, Bryan RS, et al. Fractures of the hand and wrist. In: Flynn JE, ed. Hand Surgery. 3rd ed. Philadelphia, PA: Wilkins & Wilkins; 1982:
- Schubert HE. Scaphoid fracture. Review of diagnostic tests and treatment. Can Fam Physician. 2000;46:1825-1832.
- Parvizi J, Wayman J, Kelly P, Moran CG. Combining the clinical signs improves diagnosis of scaphoid fractures. A prospective study with follow up. J Hand Surg [Br] 1998;23(3):324-7.
- Carpenter CR, Pines JM, Schuur JD, et al. Adult scaphoid fracture. Acad Emerg Med. 2014; 21(2):101-121.
- Bernard SA, Murray PM, Heckman MG. Validity of conventional radiography in determining Scaphoid waist fracture displacement. J Orthop Trauma. 2010;24(7):448-451.
- Mallee WH, Wang J, Poolman RW, et al. Computed tomography versus magnetic resonance imaging versus bone scintigraphy for clinically suspected scaphoid fractures in patients with negative plain radiographs. Cochrane Database Syst Rev. 2015;CD010023.
- Singh HP, Taub N, Dias JJ. Management of displaced fractures of the waist of the scaphoid: meta-analyses of comparative studies. Injury. 2012;43(6):933-939.
- Buijze GA, Goslings JC, Rhemrev SJ, et al. Cast immobilization with and without immobilization of the thumb for nondisplaced and minimally displaced scaphoid waist fractures: a multicenter, randomized, controlled trial. J Hand Surg Am. 2014;39(4):621-627.
- Inoue G, Shionoya K. Herbert screw fixation by limited access for acute fractures of scaphoid. J Bone Joint Surg. 1977;79(3):418-421.
- Zaidemberg C, Siebert JW, Angrigiana C. A new vascularized bone graft for scaphoid nonunion. J Hand Surg. 1991;16(3):474-478.
- OrthoInfo. Scaphoid fracture of the wrist. Available at: http://orthoinfo.aaos.org/topic.cfm?topic=A00012. Accessed on October 5, 2021.
- Kumar S, O’Connor A, Despois M, Galloway H. Use of early magnetic resonance imaging in the diagnosis of occult scaphoid fractures: the CAST Study (Canberra Area Scaphoid Trial). N Z Med J. 2005;118(1209):U1296.
- Khalid M, Jummani ZR, Kanagaraj K, et al. Role of MRI in the diagnosis of clinically suspected scaphoid fracture: analysis of 611 consecutive cases and literature review. Emerg Med J. 2010;27(4):266-269. 20.
- Smith M, Bain GI, Turner PC, Watts AC. Review of imaging of scaphoid fractures. ANZ J Surg. 2010;80(1-2):82-90.
More on Wrist Injuries
- Injuries To The Upper Extremity Due To Falls On Outstretched Hands (FOOSH)
- Galeazzi Fracture–Dislocation Of The Wrist Or Isolated Distal Radius Fracture?
- A 27-Year-Old Male With Pain After A Fall

Muhammad Asim, MBBS, FRNZCUC, FRNZCGP