Published on
Differential Diagnosis
- Early repolarization
- Hyperkalemia
- Acute pericarditis
- ST-elevation myocardial infarction
- Brugada syndrome
Diagnosis
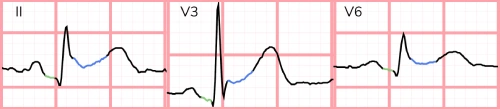
This patient was diagnosed with acute pericarditis. The ECG reveals sinus tachycardia with a rate of 108 beats per minute. There is diffuse, concave up ST-segment elevation without reciprocal changes and diffuse PR-segment depression (Figure 2).
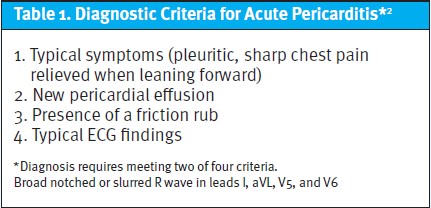
Acute pericarditis is inflammation of the pericardium, extending to the epicardium. Common causes include drugs (eg, hydralazine, penicillin), infections (eg, bacterial, viral, or fungal), malignancy, rheumatologic conditions (eg, lupus, rheumatoid arthritis, etc.), sequelae of myocardial infarction (eg, Dressler syndrome), uremia, and idiopathic.1 It is diagnosed by meeting two of four criteria (Table 1).
Differentiating pericarditis from ST-elevation myocardial infarction (STEMI) can be challenging, but the majority of cases can be accurately diagnosed with careful attention to several electrocardiographic features.
Features that suggest pericarditis over STEMI include any of the following: diffuse concave up ST-elevations without reciprocal changes, PR depression, PR elevation in aVR, ST-elevation in lead II greater than lead III, and Spodick’s sign (downsloping of the TP segment).3
The test characteristics of any single electrocardiographic feature are insufficient to rule in/out pericarditis; the feature with the highest odds ratio for predicting STEMI (over pericarditis) is reciprocal ST-depressions.
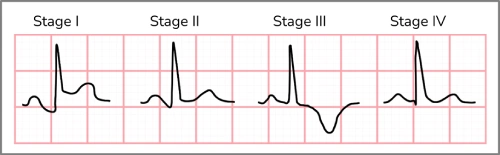
Acute pericarditis tends to follow a natural progression of electrocardiographic findings. The first 2 weeks are characterized by the aforementioned findings. Over several weeks, the ST-elevation resolves, and the T waves flatten. Next, the T waves invert. Finally, over several weeks, the ECG returns to the patient’s baseline (Figure 3).4
Treatment includes nonsteroidal anti-inflammatory medications tapered over 3-4 weeks and colchicine for 3 months. It’s also reasonable to prescribe a proton pump inhibitor to counteract the gastrointestinal side effects. Corticosteroids are reserved for patients with contraindications to initial therapy, but are not preferred as they are associated with increased recurrence.2
Early repolarization can cause similar electrocardiographic features, but this patient’s presenting symptoms make acute pericarditis the most likely diagnosis. Hyperkalemia can cause several electrocardiographic changes, but diffuse concave up ST-elevation like those seen in acute pericarditis has not been described. Brugada syndrome is a sodium channelopathy that causes characteristic ST-segment elevation in leads V1 and V2.
Additional examples may be found in the ECG Stampede glossary (www.ecgstampede.com/glossary).
Learnings/What to Look for
- Electrocardiographic features that suggest acute pericarditis include diffuse concave up ST-elevations without reciprocal changes, PR depression, ST-elevation in lead II greater than lead III, and Spodick’s sign (down-sloping of the TP segment)
- The presence of reciprocal changes or ST-elevation greater in lead III than lead II is highly suggestive of STEMI
Pearls for Urgent Care Management
- Patients with a clear diagnosis of acute pericarditis with a benign etiology and reliable follow-up can be initiated on nonsteroidal anti-inflammatory medications with or without colchicine
- If the diagnosis is in question, the etiology is unclear, or the patient lacks reliable follow-up, transfer to an emergency department
References
Mattu A, Tabas J, Brady W. Electrocardiography in Emergency, Acute, and Critical Care. 2nd ed. The American College of Emergency Physicians; 2019.
- LeWinter MM. Acute pericarditis. N Engl J Med. 2017;371(25):349-359.
- Witting MD, Hu KM, Westreich AA, et al. Evaluation of Spodick’s sign and other electrocardiographic findings as indicators of STEMI and pericarditis. J Emerg Med. 2020;58(4):562-569.
- Spodick DH. Diagnostic electrocardiographic sequences in acute pericarditis. Significance of PR segment and PR vector changes. Circulation. 1973;48(3):575-580.
Download the article PDF: A 67-Year-Old Male with Chest Pain, Dyspnea, and a History of Lung Cancer