Published on
Differential Diagnosis
- Right bundle branch block
- Non ST-elevation myocardial infarction
- Wellens syndrome
- Right heart strain
- Left ventricular hypertrophy
Diagnosis
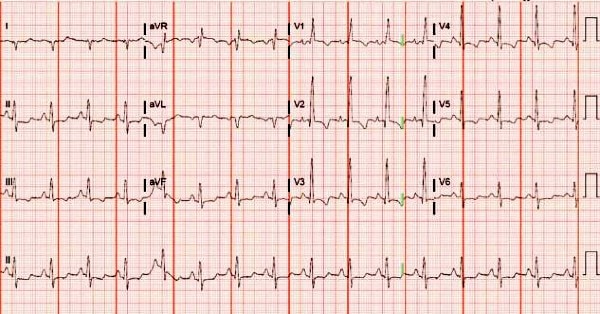
This patient was diagnosed with right heart strain. The ECG shows a regular, narrow-complex rhythm at a rate of 96 bpm. There is a right axis deviation (QRS axis >90⁰ degrees). The anterior leads (V1-V4) have T wave inversions, and ST depressions are present in the inferior leads (II, III, aVF). A dominant R wave in V1 is also present.
Together, these findings are concerning for right heart strain or right ventricular strain, a pattern seen in patients with right ventricular hypertrophy or dilatation. Any condition that causes deformation of the muscle of the right ventricle can cause these ECG findings, including but not limited to:
- pulmonary hypertension
- pulmonary embolism
- lateral myocardial infarction
- chronic lung disease such as COPD
- pulmonic stenosis
- bronchospasm1
While it is clear that right heart strain is present on this ECG, it is impossible to know from just the ECG what condition is causing this pattern. In this particular case, the patient had a pulmonary embolism causing right heart strain.
This constellation of findings can be easily confused with other conditions and should be viewed within the context of the patient’s clinical presentation. For example, patients with Wellens syndrome will classically have anterior T wave inversions whose morphology may resemble those seen in right heart strain. However, in a patient with Wellens syndrome, T wave inversion in lead III is less likely and we would expect the patient to be completely pain-free following a painful episode. Similarly, if an ECG is taken out of context or interpreted incompletely rather than as a whole, it can be easy to mistake a right ventricular strain pattern for a simple right bundle branch block or nonspecific ischemia.
Learnings/What to Look for2
Some key electrocardiographic features of right heart strain are:
- Right axis deviation
- Dominant R wave in V1
- Dominant S wave in V5 or V6
- T wave inversions and ST depressions in right precordial (V1-4) and inferior leads (II, III, aVF)
- S1Q3T3: a “classic” but not specific or sensitive finding of deep S-wave in lead I, Q wave in lead III, and inverted T wave in lead III
- Incomplete or complete right bundle branch block
- Sinus tachycardia
Pearls for Urgent Care Management
- ECGs are an important triage tool when assessing for right heart strain—they are easier to obtain than an echocardiogram or CTA, and can convey useful information to help risk stratify patients
- No one specific finding is diagnostic of right heart strain, and it is impossible to know from just an ECG what is causing the right ventricular dysfunction. Use the ECG findings as a building block to help guide your diagnosis and management, and maintain a broad differential
- Right ventricular strain pattern on ECG is associated with poor short-term outcomes in patients with pulmonary embolism and normal blood pressure3
- Initiate transfer to the ED in patients where you suspect PE with findings of right heart strain on ECG
References
- Matthews JC, McLaughlin V. Acute right ventricular failure in the setting of acute pulmonary embolism or chronic pulmonary hypertension: a detailed review of the pathophysiology, diagnosis, and management. Curr Cardiol Rev. 2008;4(1):49-592.
- Marchick MR, Courtney DM, Kabrhel C, et al. 12-lead ECG findings of pulmonary hypertension occur more frequently in emergency department patients with pulmonary embolism than in patients without pulmonary embolism. Ann Emerg Med. 2010;55(4):331-335.
- Shopp JD, Stewart LK, Emmett TW, et al. Findings from 12-lead electrocardiography that predict circulatory shock from pulmonary embolism: systematic review and meta-analysis. Acad Emerg Med. 2015;22(10):1127–1137.