Published on
Urgent message: Nonspecific presentation and time lapsed between injury and presenting to urgent care can delay diagnosis and initiation of proper management in patients ultimately diagnosed with myotendinous rupture of pectoralis major, a relatively rare injury that is becoming more common.
E. Casey Anders, Chinedum Nkemakolam, MA, and Lindsay Tjiattas-Saleski, DO
Citation: Anders EC, Nkemakolam C, Tjiattas-Saleski L. Myotendinous rupture of pectoralis major: a case report. J Urgent Care Med. 2023;17(11):21-23.
Key words: pectoralis major muscle, myotendinous rupture, rehabilitation, muscle tear
ABSTRACT
Myotendinous rupture of pectoralis major muscle is a rare injury, but its incidence is becoming more common due to the increasing popularity of strength training and contact sports. The pectoralis major muscle is responsible for adduction, flexion, and internal rotation of the humerus. It commonly ruptures when there is additional force or tension placed on a muscle that is already extended, externally rotated, and eccentrically contracted; this is a movement typically seen during a bench press. Prompt diagnosis is reported to improve patient outcomes when surgery is completed within the first 8 weeks.
CASE REPORT
A 39-year-old male presented with right shoulder pain that occurred during a workout 2 days prior. At the time of injury, he reported being on his last repetition of a bench press series with 345 pounds on the bar when he described what felt like “a braided rope being torn fiber by fiber” localized to the shoulder area. This sensation caused him to initially drop the bar, but there was no lasting pain. He later noticed weakness and found his right shoulder and upper arm to be swollen and bruised (Figure 1). At presentation, he was documented to have bruising on the right arm and chest wall, tenderness, edema, and decreased range of motion with external rotation and extension. The arm was neurovascularly intact and his pain level was rated at 7/10.

The patient reported no previous injury to this area. He has an extensive surgical history including a right knee meniscus repair in 2017, hemilaminectomy and microdiscectomy in 2018, gangrenous appendix removal in 2019, and L3-L4 fusion with prosthetic disc in 2020. His maintenance medications included gabapentin 600 mg BID, tramadol 50 mg, cyclobenzaprine 10 mg, indomethacin 50 mg BID, and acetaminophen OTC PRN. He has no pertinent past medical history. He smokes cigars daily and denies use of alcohol or illicit drugs.
DIFFERENTIAL DIAGNOSIS
Due to the location and physical presentation of the injury, a rupture of the biceps tendon, proximal humerus fracture, rotator cuff tendon tear, and shoulder dislocation should all be considered at the time of diagnosis.
OUTCOME
An MRI of the chest without contrast revealed a full thickness rupture of the right pectoralis major (Figure 2).
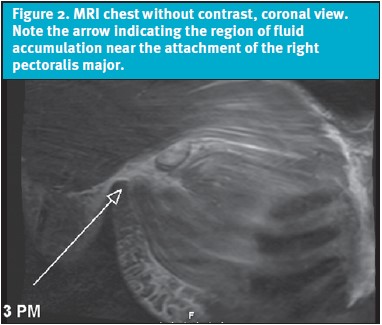
The patient was discharged home with a right pectoralis major muscle rupture diagnosis, instructed to follow up with his PCP, and referred to orthopedics.
He underwent surgical repair 22 days after initial injury.
DISCUSSION
The pectoralis major is a large, superficial muscle lying in the anterior thoracic cage. It has two heads: a sternal head originating at the sternum and first six costal cartilages, and a clavicular head originating from the clavicle.1 The muscle fibers converge onto their insertion point at the greater tubercle of the humerus via the pectoral tendon. The muscle has variation in fiber lengths, allowing it to flex, adduct, and internally rotate the humerus.2 Prior to insertion, the sternal head fibers pass underneath the clavicular head, causing them to become maximally stretched when the arm is abducted, externally rotated, and extended.3 This leaves the sternal head in a vulnerable position during motions like the bench press. Most ruptures affect the distal portion of the muscle, either at the musculotendinous junction (24% to 29%) or at the insertion site on the humerus (59% to 65%), and commonly result from direct injury or extreme muscle tension.2,3 In 2015, there were less than 400 documented cases, with 76% of them occurring after 1990.2,4
Patients generally report a tight pulling sensation or audible sound with sudden pain and weakness at the time of injury.1 They present with bruising, swelling, and cosmetic defects to the axilla, anterior chest, and upper arm on the injured side.2,5 After a tear, there is notable loss of motion and strength during internal rotation.2 Pain can be intense, but then generally subsides. Inspection of the chest wall may show unilateral bulging of the muscle or a dropped nipple, both signifying a medially retracted pectoralis major.2 Comparison of axillary folds should be performed by having the patient adduct their arms with their hands resting on their iliac crests. This will show hollowing or loss of the axillary fold.2 These exam findings should add a pectoralis major muscle tear to the differential, along with proximal biceps tendon injury, acromioclavicular joint separation, sternoclavicular joint dislocation, or rotator cuff tendon tear.
Diagnosis
Diagnosis is made clinically. Extent of the injury is confirmed with radiological imaging.6 A standard radiograph can exclude other contributing pathologies but is limited in evaluation of a pectoralis muscle injury specifically and is generally not recommended. MRI, the gold standard for diagnosis, can confirm a muscle tear, classify the type, assess the grade, and determine location of the injury.1,7 MRI was found to have a sensitivity of 73.9% and specificity of 72.2% for avulsion injuries, and a sensitivity of 75% and specificity of 79.3% for musculotendinous injuries on military populations.8 The accuracy of MRI decreases with chronic tear evaluation.9
Treatment
A pectoralis major tear can be treated surgically or conservatively. Nonsurgical treatment consists of rest, ice, analgesics, and immobilization for 3 weeks prior to physical therapy.1,4 This is recommended for sedentary, less active patients or proximal muscle belly tear injuries.11 Surgical treatment, especially when completed within the first 8 weeks, has a significantly better outcome than delayed surgical treatment or conservative treatment alone.4 There is no reported difference in patient outcome based on type of surgical repair.12 Surgery is typically recommended for young, active patients in the context of both acute and chronic ruptures.
Postoperative rehabilitation should focus on restoring range of motion and re-establishing strength and stability to the muscle. High weight, low repetition exercises involving the pectoralis major discouraged.2 Consensus on rehabilitation protocols is lacking in current literature, but it was found that patients wait about 4 weeks postsurgery before beginning rehabilitation exercises.5 This study also found that 90% of surgically repaired injuries returned to sport 6 months postsurgery. Of those able to return, 74% performed at the same level prior to injury.5
CONCLUSION
This case report presents a confirmed case of a myotendinous tear of the sternal head of the right pectoralis major muscle. This injury seldom occurs, has a nonspecific physical presentation, and can present several days after initial injury, which can lead to a delay in the initiation of proper management. Obtaining a proper imaging study, such as an MRI, is a useful tool to confirm the diagnosis and determine the extent of muscle damage. Among the treatment options, prompt surgical intervention has been shown to result in the best patient outcomes.
Ethics statement: The patient consented to the submission of this case report to the journal.
Manuscript submitted March 16, 2023; accepted April 27, 2023.
References
- Metzger PD, Bailey JR, Filler RD, et al. Pectoralis major muscle rupture repair: technique using unicortical buttons. Arthrosc Tech. 2012;1(1):119-125.
- Haley CA, Zacchilli MA. Pectoralis major injuries. Clin Sports Med. 2014;33(4):739-756.
- Kakwani RG, Matthews JJ, Kumar KM, et al. Rupture of the pectoralis major muscle: surgical treatment in athletes. Int Orthop. 2006;31(2):159-163.
- Bak K, Cameron EA, Henderson IJ. Rupture of the pectoralis major: a meta-analysis of 112 cases. Knee Surg Sports Traumatol Arthrosc. 2000;8(2):113-119.
- Yu J, Zhang C, Horner N, et al. Outcomes and return to sport after pectoralis major tendon repair: a systematic review. Sports Health. 2018;11(2):134-141.
- Chiavaras MM, Jacobson JA, Smith J, Dahm DL. Pectoralis major tears: anatomy, classification, and diagnosis with ultrasound and MR imaging. Skeletal Radiol. 2014;44(2):157-164.
- WikiSM. Pectoralis major injuries. Available at: https://wikism.org/Pectoralis_Major_Injuries. Accessed August 2, 2023.
- Synovec J, Shaw KA, Hattaway J, et al. Magnetic resonance imaging of pectoralis major injuries in an active duty military cohort: mechanism affects tear location. Orthop J Sports Med. 2020;8(6):232596712092501.
- Chang ES, Zou J, Costello JM, Lin A. Accuracy of magnetic resonance imaging in predicting the intraoperative tear characteristics of pectoralis major ruptures. J Shoulder Elbow Surg. 2016;25(3):463-468.
- Marsh NA, Calcei JG, Antosh IJ, Cordasco FA. Isolated tears of the sternocostal head of the pectoralis major muscle: surgical technique, clinical outcomes, and a modification of the Tietjen and Bak classification. J Shoulder Elbow Surg. 2020;29(7):1359-1367.
- Petilon J, Carr DR, Sekiya JK, Unger DV. Pectoralis major muscle injuries: evaluation and management. J Am Acad Orthop Surg. 2005;13(1):59-68.
- Bodendorfer B, McCormick B, Wang D, et al. Treatment of pectoralis major tendon tears: a systematic review and meta-analysis of operative and nonoperative treatment. Orthop J Sports Med. 2020;8(7_suppl6):2325967120S0041.
Author affiliations: E. Casey Anders, OMS III, VCOM-Carolinas. Chinedum Nkemakolam, OMS III, VCOM-Carolinas. Lindsay Tjiattas-Saleski, DO, VCOM-Carolinas. The authors have no relevant financial relationships with any commercial interests.
Read More
- Physical Therapy As Nonsurgical Management And Presurgical Management Of Most Common Knee Pathologies
- When X-Rays Lie: Important Orthopedic Diagnoses To Consider With Normal Imaging
- An Uncommon Mechanism Of Work-Related Partial-Thickness Triceps Tear
Download the article PDF: Myotendinous Rupture of Pectoralis Major: A Case Report