Published on
Urgent message: Musculoskeletal pain is a common urgent care complaint, with x-rays very commonly ordered. However, a “normal” image does not necessarily support eliminating what could be a serious injury from the differential diagnosis.
Arun Sayal, MD, CCFP(EM)
Citation: Sayal A. When X-Rays Lie: Important Orthopedic Diagnoses to Consider with Normal Imaging. J Urgent Care Med. 2022;16(7):13-16.
Medical tests lie. Not intentionally, of course, but their result may not align with reality. A test may be positive in the absence of pathology (a false positive); conversely, a test may be negative in the presence of pathology (a false negative). At the end of the day, the purpose of any testis not to make a diagnosis, but to add data to our pretest probability. All test results (positive or negative) must be placed in the clinical context of each particular patient.
One example of these principles is the ability of an electrocardiogram to diagnose disease. An ECG is a very good test—but it’s not enough to definitively rule out serious pathology, such as acute coronary syndrome; in fact, for an acute myocardial infarction the first ECG is diagnostic only 13% to 69% of the time,1 with 13% being diagnosed on serial ECGs.2
Just as an ECG may “lie,” so can an x-ray.
A common orthopedic pitfall is using the x-ray as the sole tool to rule in or rule out a diagnosis. For emergency departments, one of the most common causes of medical error is misdiagnosis, and the most common misdiagnoses are orthopedic.3
A typical approach for any chief complaint is to incorporate the possible diagnoses with the patient’s history of present illness, age, past medical history, physical exam, tests, and response to treatment to reach a reasonable conclusion about the presumptive diagnosis. Yet, for some reason, urgent care and emergency medicine physicians tend to do things differently for orthopedic patients by over-relying on the radiograph: A positive x-ray equates to a fracture or dislocation; a negative x-ray may equate to a soft-tissue injury (unless the patient has snuffbox tenderness, in which case the diagnosis becomes a “clinical scaphoid” fracture).
Clearly, this commonly used algorithm is deeply flawed. With a normal x-ray, numerous important diagnoses remain possible.
The mnemonic to help us remember these important diagnoses is: SCAReD OF
S – Septic joint
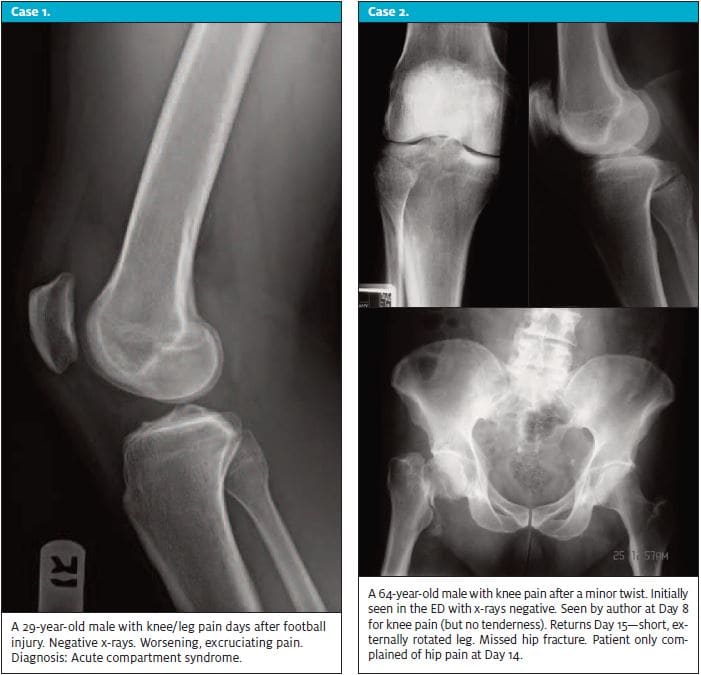
C – Compartment syndrome
A – Abuse
Re – REferred pain/REport is false
D – Dislocation/subluxation
O – Operative soft-tissue injury
F – Fracture
Septic joint – Be cautions if this is an atraumatic joint pain and if there is swelling in an immunocompromised patient. Consider any immunosuppressive drugs (prednisone, antirheumatologic drugs, monoclonal antibody treatment, chemotherapy) or if the patient has had recent orthopedic surgery. Postoperative orthopedic wound infections often connect to a joint or to metal (a plate)—and both are serious. Refrain from administering antibiotics until the joint is tapped (unless the patient is systemically unwell), as pre-aspiration antibiotics significantly sterilize the culture. From an urgent care setting, suspected infected joints should be referred to the ED.
Compartment syndrome – This is a rare diagnosis, and one commonly missed. Seventy percent are associated with a fracture, but 30% are not.4 Other causes include a tight cast, anticoagulation, infections, crush injuries, high-pressure injection injuries, etc. Young adult males are at highest risk due to the large muscle bulk, tight fascia, and incompetent risk assessment skills. Comparing the compartment to the unaffected limb may help establish a baseline for “normal” in specific patients. The 5Ps for compartment syndrome (pain, pallor, paresthesias, paralysis, pulselessness) may be present, but paralysis and pulselessness are very late signs, manifesting when the outcome may not be reversible. The 5Ps of compartment syndrome should be: pain, pain, pain, pain, and pain. Then, look for progressive paresthesias.
Acute compartment syndrome is rare in the ED, and present even less commonly in urgent care. Always suspect compartment syndrome when pain is out of proportion to what is expected.
Abuse – When we see a fracture in a child, consider nonaccidental trauma (NAT). Certain fractures, including spiral fractures and multiple rib fractures in infants or toddlers, heighten our suspicion. There is evidence that if we miss abuse as the cause, the violence tends to recur and escalate in both frequency and severity.5
Referred pain – Thisis easily missed. One example is the child with hip pathology who presents with knee pain. Failure to examine the joint proximal and the joint distal will miss the actual diagnosis in this example; a slipped capito (upper) femoral epiphysis (SCFE/SUFE). Another example is elbow pain that can come from the a cervical radiculopathy. The clinical clue is an inability to reproduce the pain on physical exam. Another classic example of this is referred shoulder pain from acute coronary syndrome. The purpose of the physical exam is to confirm what we suspect on history.
One important caveat is in patients with chronic pain, such as elderly patients with osteoarthritis. While they may present with acute knee pain, the pain reproduced with palpation may represent their chronic pain, and not the acute source of pain.
Report is false – If there is an abnormality on a plain film, there is a chance for a radiology miss.6 By all means, look at the radiologist’s report if it is present, but also look at the plain films, especially if the report is not consistent with your suspicion. We have a history and a physical. We have a pretest probability of pathology. We know where they are tender. With that clinical information, we may have better eyes to find subtle abnormalities than our radiology colleagues.
Dislocation/subluxation – If a joint is dislocated, there is no contact between the articular surfaces. If a joint is nonanatomic, but there remains some contact of the articular surfaces, then this is termed a subluxation. (Essentially, a subluxation is a “partial dislocation,” but this is not a medically acceptable term). Subluxations, and less often dislocations, may spontaneously reduce. On history, the patient often describes the joint as having “slipped out.” In these cases, the x-ray would be normal. While the diagnosis is suspected on history, it may be further confirmed on careful physical examination (ligament testing) of the joint.
Operative soft-tissue injury. Most soft-tissue injuries are treated nonoperatively, but certain soft-tissue injuries may be operative at a later time, such as with a tear of the anterior cruciate ligament (ACL) or a meniscus tear. A minority of soft-tissue injuries are definitely surgical, with harm caused by a delay in surgical management, such as in a distal biceps rupture, patellar tendon rupture, or a quadriceps tear. These definitively surgical soft-tissue injuries need consideration at first assessment. They are joint-specific and clinical concern is based on the context of the case. If the radiograph is negative for fracture but clinical concern remains for an operative soft-tissue injury, then management involves either early surgical referral, additional imaging, or immobilization and early reassessment for confirmation.

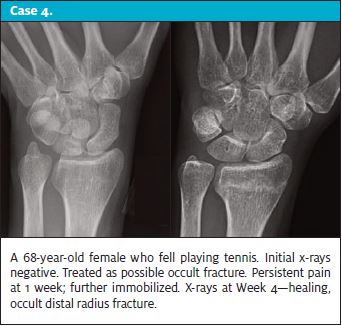
Fracture (radiographically occult) – About 20% to 30% of scaphoid fractures may not be seen on initial x-rays. It is often a clinical diagnosis; it is important to assess for appropriate signs and symptoms in a patient with normal x-rays. Among all fractures, about 5% of acute fractures do not appear on initial x-rays. In addition to scaphoid fractures, this rate is higher for pediatric growth-plate fractures, for stress fractures, and for the elderly (whose inherent osteoporosis renders fractures more likely and often challenging to see radiographically); for example, 5% of hip fractures are radiographically occult. With a relatively high pretest probability for a fracture and normal x-rays, the possibility of a fracture remains. Appropriate management for suspected fractures varies from more time (immobilization for the less serious suspected injury with ensure serial assessment) to more tests (advanced imaging for the more serious suspected injury). A patient with a clinically suspected scaphoid fracture may be immobilized and serially assessed and imaged. A patient with a clinically suspected hip (or C-spine) fracture, should have advanced imaging.
In conclusion, just as we use a reasonable approach with all chief complaints, we need to also use this same approach for the assessment of musculoskeletal injuries.
Take-Home Points
- Don’t let a normal x-ray be the sole indication to abandon clinical concern.
- Consider the history and physical before relinquishing concern.
- If the pretest probability is not suggestive of more serious pathology, then negative imaging may allow for expedient discharge and expectant management.
- If the pretest probability does suggest more serious pathology, then a negative x-ray should not definitively exclude the diagnosis.
- Remember the SCAReD OF mnemonic; in doing so, one will be less likely to be fooled by a normal ED extremity x-ray.
References
- Speake D, Terry P. First ECG in chest pain. Emerg Med J. 2001;18(1):61-62.
- Fesmire F, Percy RF, Bardoner JB, et al. Usefulness of automated serial 12-lead ECG monitoring during the initial emergency department evaluation of patients with chest pain. Annals Emerg Med. 1998;31(1):3-11.
- Brown TW, McCarty ML, et al. Closed ED claims from a US database of malpractice insurers. Acad Emerg Med. 2010;17(5):553-560.
- McQueen MM, Gaston P. Court-Brown C. Acute compartment syndrome: who is at risk? JBJS (Br). 2000;82(2):200-203.
- King WK, Kiesel EL, Simon HK. Child abuse fatalities: are we missing opportunities for intervention? Ped Emerg Care. 2006.22(4):211-214.
- Berlin L. Radiologic errors, past, present and future. Diagnosis. 2014;1(1):79-84.
Author affiliations: Arun Sayal, MD, CCFP(EM), Emergency Department and Fracture Clinic, North York General Hospital; Department of Family and Community Medicine, University of Toronto (Canada). The author is the creator and director of CASTED, a series of hands-on orthopedic courses. He otherwise has no relevant financial relationships with any commercial interests
