Published on
Urgent message: Much has been written about the integration of occupational medicine into urgent care practice. However, doing so successfully requires consideration of many important factors. This is the first in a series of articles that will examine occupational medicine in the urgent care setting from the financial and practice management viewpoint, with the aim of guiding the urgent care decision-maker and practitioner in the best practices of business and clinical occupational medicine practice.
Max Lebow, MD, MPH, FACEP, FACPM
Introduction
Occupational medicine is a branch of preventive medicine. In practice, it is generally divided into workers compensation; the treatment of workplace illnesses and injuries; and occupational health, a broad field which includes workplace wellness and injury prevention, fit-for-duty and specialty physicals (eg, Department of Transportation), and drug and alcohol testing. While these disciplines are usually closely linked, they differ in actual practice and management and will be discussed separately.
Synergy of Urgent Care and Occupational Medicine.
Urgent care and occupational medicine share many qualities of medical care and treatment. Most workplace injuries consist of minor trauma, similar to urgent care in both cause and treatment. However, it is the differences in handling that make occupational medicine a natural companion to urgent care.
Urgent care and occupational medicine can be synergistic. While urgent care is typically a morning and evening business, occ med physicals, re-checks and drug tests can be scheduled for the slower times of the afternoon to level patient ebb-and-flow and maximize productivity of a center’s providers and staff. It is often a financial challenge to keep providers and staff productive during all daily hours of clinic operations. Occupational medicine provides a balance in that its busiest hours are during the day when urgent care is slowest, and vice versa. This allows even busier clinics to add occupational medicine to their menu of services without having to increase staff. Further, occupational medicine complements urgent care not only on a daily basis, but seasonally as well. And whereas urgent care is busiest in the winter months (eg, associated with flu and flu symptoms), occupational medicine is busiest during the summer months when companies are hiring and construction projects are in full swing.
Taken together, the combination of urgent care plus occupational medicine tends to smooth out the census graph throughout the day. Figure 1 illustrates how urgent care and occupational medicine are complimentary at Reliant Immediate Care in Los Angeles, which due to an airport location is accessible to many large employers in the transportation industry which require compliance physicals and drug screenings. The airport location results in urgent care being busiest in the evening hours, with employers sending occ med cases in the morning.
As you can see, the occupational medicine patients can help smooth out the patient census over the course of a day.
The Value Proposition of Occupational Medicine
There are about 3 million workplace injuries and illnesses in the U.S. each year. Injury rates tend to be highest in the transportation, warehousing, construction, and manufacturing industries, as well as with municipal employers like police, fire, sanitation, and parks/recreation. Depending on which industry is using your clinic, there could be between 3 and 7 injuries per 100 employees. And even in industries in which injury rates are low, client businesses still need basic occupational health services, such as preplacement physical examinations, fitness for duty exams, and drug screens.
The Cascade of Occupational Medicine: Compelling Economic Rationale
Once an urgent care patient has been registered, treated, and discharged, that’s often the end of the encounter. In clear distinction from urgent care, discharge of the occupational medicine patient from their first work comp visit begins a cascade of follow-up care and case management, ancillary services (especially physical therapy), medication, and DME services. (See Figure 2.) Each episode of care, even follow-up for physical therapy, and medications/DME represent additional revenue opportunities for the clinic. And whereas workers comp and urgent care visits are reimbursed by third parties (either insurance or the government), occ med services like physicals and drug screens are paid by employers directly under NET/15 terms, enabling quick and ready cash flow for a center versus insurance accounts receivable which can take 45 to 60 days or longer to collect.
The Work Comp Cascade
New injury/illness visit to the clinic
Initial medical management of occupational medicine patients differs little from urgent care treatment. Wound care, musculoskeletal injuries, basic fracture care, and contact dermatitis are treated similarly. Perhaps the greatest difference goes to causation—workers comp expects a provider to opine on whether an injury was caused by employment, which means effective occ med providers get out and see their client’s businesses. Workers compensation providers must also be mindful of OSHA regulations that make certain activities such as allowing time off work or prescribing certain drugs as “recordable,” which can affect a client’s workers compensation insurance premiums. Many workers compensation providers thus take a conservative approach to treatment—work hardening through light/modified duty and physical therapy in lieu of surgery or prescription drugs.
Over the long run, workplace new injuries will carry higher revenue in many cases for two reasons: First, workplace injuries and trauma are more likely to also have associated procedures such as sutures, or a diagnostic test such as an x-ray. Some states even allow acupuncture and chiropractic for workers comp, which can be integrated into the urgent care/occ med practice as well as specialty services like orthopedics, hand surgery, and physiatry (physical medicine). And some providers further provide impairment examinations that assess a patient’s total disability from a workplace incident.
By contrast in urgent care, in states where case rates and managed-care predominate, many urgent care visits carry a case- or flat-fee reimbursement rate, regardless of what is done during the visit. In work comp cases, the work comp fee schedule is more likely to reimburse fee-for-service for all procedures performed and documented. The combination of trauma-related visits and the work comp fee schedule tends to bring the reimbursement for initial work comp injury treatment to about 30% over the average urgent care visit reimbursement in most clinics, in our experience. Fee schedules can differ significantly by state, as they’re typically set not by carriers, but by state industrial commissions.
In urgent care, the patient is referred back to their primary care physician at the end of a typical visit. For work-related injuries, patients are referred back to the urgent care/occupational medicine clinic for follow-up until the patient is deemed able to return to work.
Workplace Injury Follow-Up Care
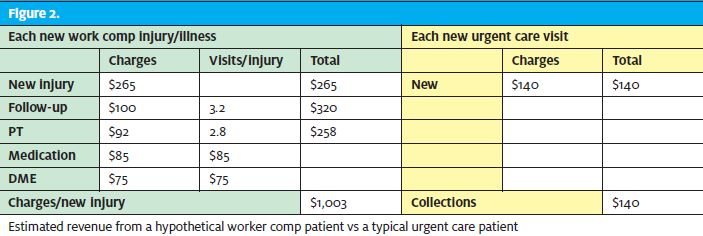
My experience is that workplace injuries require about 3.2 follow-up visits for each new injury treated, on average in our clinic. Some new injuries may be so minor that they do not require any follow-up, while others will require weeks of recovery and treatment. For purposes of forecasting, these work-related injury follow-up cases can be estimated to about 80% reimbursement of the new patient average urgent care visit.
Physical therapy
Our recommendation is for urgent care/occupational medicine clinics to bring physical therapy in-house as soon as possible, for several reasons.
First, having PT in-house improves the quality of care for the injured patient. Many patients can be improved by “work hardening” as opposed to surgery or drugs, which enables them to heal faster and return to work more quickly. Communication between the physical therapist and the treating physician is key to identifying patients whose recovery may be delayed. Time off of work, not medical, is typically the employer’s greatest expense of workplace injuries. Involvement of a physical therapist can result in earlier changes in treatment course, in earlier diagnostic testing, or referral to a specialist.
The second reason to bring physical therapy in-house is for convenience and employer/employee satisfaction. Businesses are looking for a one-stop solution to their workplace injury issues. Additionally, physical therapy can be used for occ med testing, such as demonstrating lift techniques, which is an additional cash service.
Finally, physical therapy, if done correctly, can generate revenue for the clinic. In an active occupational medicine clinic like ours, there is usually about 2.8 physical therapy visits per new injury. Properly billed, and depending on the state work comp fee schedule, physical therapy should reimburse at about 65% of a typical urgent care new visit
Medication and durable medical equipment
This is a rapidly evolving area of occupational medicine. Regardless of any changes the marketplace may undergo, there will always be a need for injured workers to get their medication and DMEs dispensed at the time of service. Negotiation with pharmacy benefit plans is a must to retain the ability to get patients what they need, when they need it. State workers comp legislation plays a role, as well.
Putting It All Together
All told, worker comp patients are likely to become more frequent and more lucrative than a “typical,” straightforward urgent care patient. The sheer complexity of the process makes for a more formal and long-lasting relationship between patient and provider.
As described previously, adding occupational medicine to an existing urgent care practice can help improve efficiency and help meet the fixed costs of the practice by keeping staff busy across all hours of operation. This is important given that labor, and especially provider labor, is the greatest expense in urgent care.
What is learned from the occupational medicine cascade is that for each new workplace injury treated in the clinic, in terms of income, revenue can be expected to equal or surpass the revenue generated from up to seven urgent care visits, factoring follow-up visits, physical therapy, and medication and DME into the reimbursement mix. This means that even a modest program (say, 50 new injuries per month, less than 2 new injuries per day), can generate enough revenue to convert a struggling practice into one that is solidly in the black.
Next Steps
So, let’s get started, right? Not so fast. To have a successful and long-term occupational medicine program, the clinic will need basic marketing; providers who understand the active management of occupational medicine illness and injuries and proper documentation; and a commitment to quality of care and occupational medicine that is defined by its own parameters of success. In our next articles, we will discuss the elements of a successful occupational medicine program, so providers and clinic operators alike can make the transition to offering occupational medicine as smoothly and efficiently as possible.
