Published on
Urgent message: Urgent care and emergency department visits focus on acute clinical conditions, with an emphasis on timely administration of medications. Patients discharged outside the typical service hours of a community pharmacy may not have access to a 24-hour pharmacy and have to return home without their prescription medication, creating additional barriers to prescription adherence for patients.
Emilie M. Collongette, PharmD, BCMTMS; Sara Panella, PharmD, BCPS; Michael A. DeCoske, PharmD, BCPS; Ernesto Sanz Martinez, MD
Citation: Collongette EM, Panella S, DeCoske MA, Martinez ES. Evaluating abandonment of urgent care prescriptions sent to an automated drug dispenser vs a community pharmacy: a retrospective cohort study. J Urgent Care Med. 2023;17(7):27-33.
Key words: prescription, automated dispensing, point-of-care dispensing
ABSTRACT
Introduction: This study sought to determine the rate of prescription abandonment of urgent care (UC) prescriptions sent to an automated drug dispenser vs a community pharmacy. Automated drug dispensers, located on-site within the UCs, provide point-of-care (POC) dispensing throughout the UC’s hours of operation. Patients who do not have access to POC UC automated drug dispensers and are discharged outside the typical service hours of a community pharmacy may have to return home without their prescription medication, creating additional barriers in ensuring prescription adherence.
Methods: A retrospective chart review was conducted of patients discharged from a high-volume single-center UC from January 1–June 30, 2021. Patients were randomized 1:1 based on dispensing site selection: automated on-site drug dispenser or community pharmacy. Eligible prescriptions were based on the automated drug dispenser formulary.
Results: A total of 350 patient charts were reviewed, with 334 prescriptions sent to the automated drug dispenser and 324 prescriptions to a community pharmacy. Prescription abandonment occurred in six prescriptions (2%) sent to the automated drug dispensers compared with 74 prescriptions (23%) sent to a community pharmacy (p<0.001). The occurrence of an additional acute care visit within 30 day of urgent care discharge was two times greater among patients with prescription abandonment (18% vs 9%, p=0.05).
Conclusion: In patients discharged from the UC, the use of the automated drug dispenser led to a significant reduction in the rate of prescription abandonment. Presenting patients with the opportunity for POC pharmaceutical dispensing increases the likelihood of same-day prescription pick up.
INTRODUCTION
Prescriptions received electronically, via fax, telephone or hand-delivered to a dispensing pharmacy that are not retrieved by a patient are considered abandoned.1,2 Factors potentially contributing to prescription abandonment include: perception of medication as unnecessary, medication-related concerns, cost, pharmacy wait times, and lack of time.3,4 Prescription abandonment, primary medication nonadherence, often leads to suboptimal patient outcomes and preventable healthcare spending.5 A 2018 study found the rate of prescription abandonment among emergency department (ED) prescriptions to be 11.5%.6
Urgent care (UC) and ED visits focus on acute clinical conditions, with an emphasis on timely administration of medications. Timely initiation and maintenance of therapy allows for optimal patient outcomes and therapeutic effects. Patients may be limited in their ability to fill prescriptions at a community pharmacy when discharged from the UC given visits are often unplanned and may occur outside of normal business hours. The automated drug dispenser provides point-of-care dispensing throughout the UC’s hours of operation. Patients discharged outside the typical service hours of a community pharmacy may not have access to a 24-hour pharmacy and have to return home without their prescription medication, creating additional barriers in ensuring prescription adherence.
Automated drug dispensers are designed to provide prescription medications at the point-of-care. Prescription fulfillment can follow either a pharmacist or prescriber dispensing model.
Prescriber dispensing models must comply with and are subject to state rules and regulations. Following the prescriber dispensing model, automated drug dispensers are prestocked with a set formulary of medications. The prescription bottles are stocked based on medication, strength, and quantity. Patient-specific directions for use will be printed at the time of dispensing.
Patients are presented with the choice to have their prescriptions filled at the automated drug dispenser during the consultation. If the automated drug dispenser is selected, the prescription is electronically sent to the dispenser and the patient can retrieve their prescribed medications at discharge. Prescribed medications must be dispensed in a container which bears the following information in compliance with federal regulation: prescribing practitioner’s name, patient’s name, date dispensed, name and strength of medication, and directions for use.
Prior studies evaluating the use of an automated drug dispenser in the ED have shown a reduction in the rate of prescriptions abandonment.7 Limited evidence is available regarding abandonment of UC prescriptions. The primary objective of this study was to evaluate the rate of prescription abandonment of UC prescriptions sent to an automated drug dispenser vs a community pharmacy.
METHODS
All methods were approved by the Baptist Health South Florida Institutional Review Board quality committee. The primary outcome, prescription abandonment, was defined as prescriptions not retrieved within 14 days of the written date. The secondary outcomes analyzed prescription dispensing site based on the time of UC discharge and the occurrence of an acute care visit (UC, ED, observation, or admission) within 30 days of UC discharge.
STUDY CHARACTERISTICS
This is a retrospective cohort study that examined abandonment of UC prescriptions sent to an automated drug dispenser vs a community pharmacy. Medical records of patients discharged from a high-volumesingle-center UC were screened to a set of inclusion and exclusion criteria from January 1 to June 30, 2021.
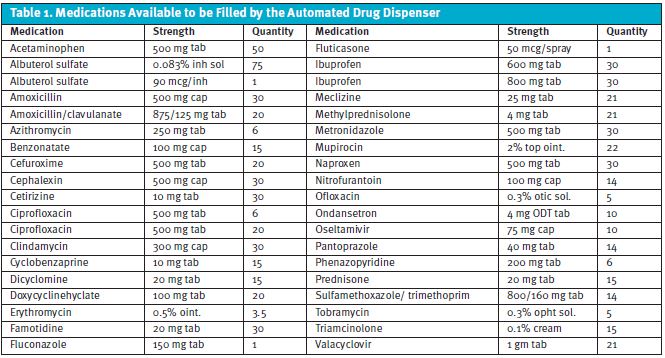
Inclusion criteria consists of the following: adults 18 years or older with at least one discharge prescription included in the automated drug dispenser formulary (Table 1).
Exclusion criteria consists of the following: a patient’s discharge prescriptions were sent to multiple dispensing locations, or the community pharmacy external fill history was not available. Medical records were stratified into two cohorts based on dispensing site selection: automated drug dispenser and community pharmacy. All patient identifiers were removed, and participants were given identification numbers. Randomization was used to identify 175 participants from each cohort. The data reviewed included participant’s demographics, visit documentation, prescription details, external fill history, and additional acute care visit encounters. Data were stored electronically on a password-secured drive.
Prescriptions were considered abandoned if they were not retrieved within 14 days of the written date. A report of prescriptions sent to the automated drug dispenser was generated to determine the dispensing outcome. A feature integrated into the electronic health record provided external fill history data for participating community pharmacies. The date of prescription pick-up, if applicable, was available for both dispensing sites.
The primary objective was to determine if the rate of prescription abandonment differed among UC prescriptions sent to an automated drug dispenser vs a community pharmacy.
The secondary objectives were to analyze trends in dispensing site selection based on the time of UC discharge and the occurrence of acute care visits (UC, ED, observation, or admission) within 30 days of UC discharge among patients who retrieved their prescriptions vs those who abandoned their prescriptions.
STATISTICAL ANALYSIS
It was determined that a sample size of 350 patients was needed to detect a difference between the groups. Fisher’s exact was utilized to assess if demographic data corresponded to a significant difference between both groups. Chi square test was used to determine the statistical difference between categorical variable (rate of prescription abandonment, time to prescription pick up, occurrence of readmission). P-values are reported. Descriptive statistics were also used to evaluate trends in the data collected. Graphs were created for visualization.
RESULTS
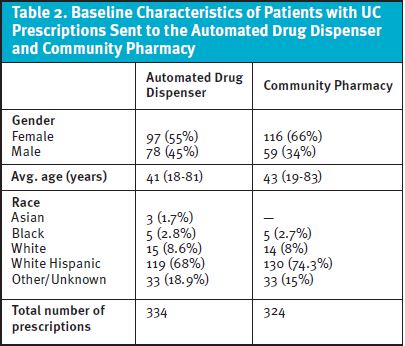
A total of 350 patient charts were reviewed—175 patients with prescriptions sent to the automated drug dispenser and 175 patients with prescriptions sent to a community pharmacy. Baseline characteristics and are outlined in Table 2.
A total of 334 prescriptions were sent to the automated drug dispenser vs 324 prescriptions that were sent to a community pharmacy.
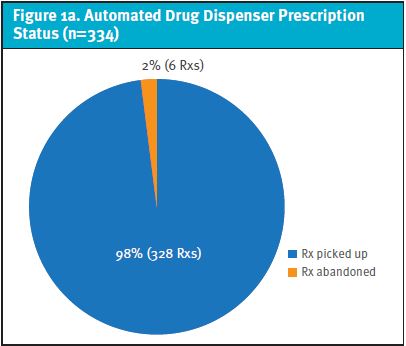
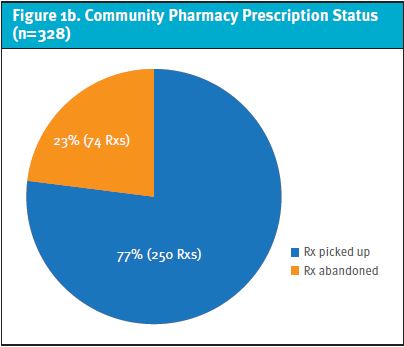
Of the prescriptions sent to the automated drug dispenser, six prescriptions (2%) were abandoned compared with 74 prescriptions (23%) sent to a community pharmacy (p <0.001) (Figure 1a and 1b). Same-day pick-up occurred for 328 prescriptions (98%) sent to the automated drug dispenser vs 202 prescriptions (62%) of the prescriptions sent to a community pharmacy (p<0.001).
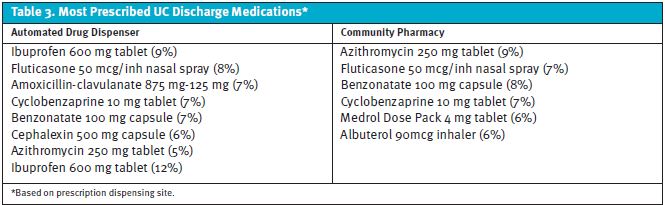
The prescriptions abandoned at the automated drug dispenser were: famotidine 20 mg oral tablet,fluticasone 50 mcg/inh nasal spray, ibuprofen 600 mg oral tablet, mupirocin 2% topical ointment, naproxen 500 mg oral tablet,and ondansetron 4 mg oral disintegrating tablet.
The most common prescriptions abandoned at a community pharmacy were: ibuprofen 600 mg tablets (16%), fluticasone 50 mcg/inh nasal spray (12%), albuterol 90 mcg inhaler (7%), and azithromycin 250 mg tablet (7%).
The most commonly prescribed medication among both groups was ibuprofen 600 mg tablets (Table 3).
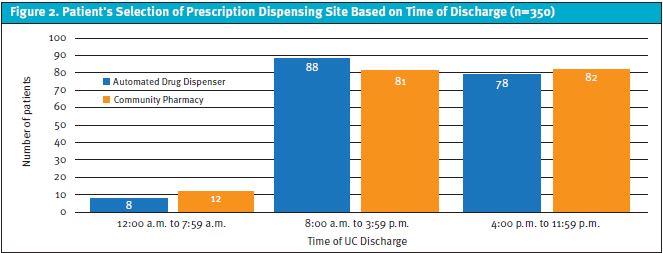
Prescription dispensing site selection was analyzed based on the time of UC discharge (Figure 2). Between the hours of 12:00 am and 7:59 am, eight patients selected the automated drug dispenser and 12 patients a community pharmacy. Between 8:00 am and 3:59 pm, 88 patients selected the automated drug dispenser and 81 patients a community pharmacy. Between 4:00 pm and 11:59 pm, 79 patients selected the automated drug dispenser and 82 patients a community pharmacy. The majority of patients (94%) were discharged between 8:00 am and 11:59 pm. There were 59 unique community pharmacies selected by the 175 patients reviewed; of those, three community pharmacies received 41% of the prescriptions.
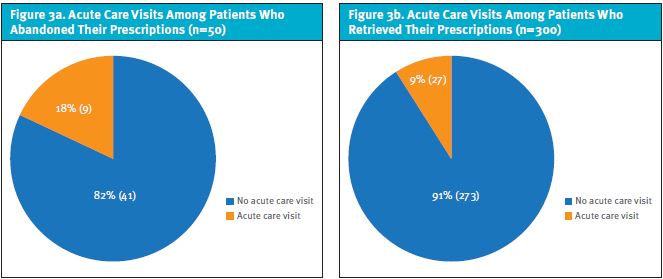
The occurrence of an acute care visit within 30 days of discharge was compared based on prescription pick-up status, independent of the dispensing site. Out of the 350 patient charts reviewed, 300 patients retrieved their prescriptions, and 50 patients abandoned their prescriptions. Twenty-seven of the 300 patients (9%) who retrieved their prescriptions from either the automated drug dispenser or a community pharmacy had at least one additional acute care within 30 days of UC discharge compared with nine of the 50 patients (18%) who abandoned their prescriptions (p=0.05) (Figure 3A and 3B).
DISCUSSION
The goal of this study was to determine if the rate of prescription abandonment differed among UC prescriptions sent to an automated drug dispenser vs a community pharmacy.
A total of 658 prescriptions were reviewed. Prescriptions included were based on the automated drug dispenser formulary (Table 3) to allow for a direct comparison. Only those patients who sent all discharge prescriptions to the same dispensing site were included to eliminate any potential differences among dispensing site selection and study outcomes.
The rate of prescription abandonment was significantly lower for prescriptions sent to the automated drug dispenser. Only six prescriptions (2%) were abandoned, compared with 74 prescriptions (23%) sent to a community pharmacy (p<0.0001).
When analyzing the rate of prescription abandonment among the prescriptions solely available behind-the-counter, the rate of prescription abandonment continued to be significantly lower among those sent to the automated drug dispenser 0.89% (three) compared to 13% (42) sent with a community pharmacy (p<0.001). Therefore, the data show that inclusion of over-the-counter prescriptions did not sway the results of the study.
The use of the automated drug dispenser in our study showed to decrease the rate of prescription abandonment and the time to prescription pick-up.
The rate of same day pick-up was significantly greater among prescriptions sent to the automated drug dispenser (98% vs 62%, p<0.001). Subanalysis of the study results to review antimicrobial therapies was also performed, and found that 100% of antibiotics prescriptions sent to the automated drug dispenser were retrieved same-day compared with 54% of the antibiotic prescriptions sent to a community pharmacy (p<0.001). Furthermore, 25% of antibiotic prescriptions sent to a community pharmacy were retrieved next-day, 4% within 2 to 7 days of written date, and 17% were abandoned. The rate of same-day pick-up for antibiotic prescriptions was significantly greater in the prescriptions sent to the automated drug dispenser vs a community pharmacy, demonstrating the positive impact the use of automated dispenser can have on time-sensitive prescriptions.
Prescription dispensing site-selection was analyzed based on the time of UC discharge. There was no significant correlation noted between time of UC discharge and dispensing site selection. Of the 59 community pharmacies, the three most common community pharmacies were located within 1.5 miles of the UC and received 133 prescriptions (41%). The hours of operations for these pharmacies were 24 hours, 7:00 am–12:00 am, and 8:00 am to 8:00 pm. The difference in pharmacy operation hours reflected by the three most commonly selected pharmacies presents an additional factor patients must consider when selecting a community pharmacy vs the automated drug dispenser.
Between the hours of 12:00 am and 7:59 am, eight patients selected the automated drug dispenser and 12 patients a community pharmacy.
None of the prescriptions sent to the automated drug dispenser were abandoned, whereas 23% of the prescriptions sent to a community pharmacy were abandoned (p<0.001). The significant reduction of prescription abandonment associated with the use of automated drug dispenser in patients discharged between the hours of 12:00 am and 7:59 am should be taken into consideration by providers when presenting the opportunity for point-of-care dispensing. Furthermore, only three of the community pharmacies that received prescriptions between 12:00 am and 7:59 am were open at the time of UC discharge, illustrating pharmacy operating hours may be a barrier to prescription pick-up.
In addition, our study looked to assess the rate of an additional acute care visit within 30 days of UC discharge within the health system.
The occurrence of an additional acute care visit was two times greater among patients with prescription abandonment (18%) compared with patients who retrieved their prescription (9%) (Figure 3A and 3B). The rate of an acute care visit within 30 days of UC discharge between patients with prescription abandonment and pick up was not statistically significant. Of the patients with prescription abandonment and an additional acute care visit, 67% had the same or a related diagnosis code to that of their original UC visit.
The Agency for Healthcare Research and Quality (AHRQ) reported that in 2018, there were 3.8 million adult hospital readmissions within 30 days, with an average readmission rate of 14%.8 The readmission rate among our study participants with prescription abandonment was higher than the reported 2018 average. Therefore, UC stakeholders may consider the correlation between prescription abandonment and readmission rates as an aim to promote the use of the automated drug dispenser to help reduce additional acute care visits, given its significant reduction in prescription abandonment.
LIMITATIONS
The study demonstrated that the use of the automated drug dispenser led to a lower rate of UC prescription abandonment, but did have limitations. As a single-center study, the results may not be generalizable to all UC settings. The study population was representative of the area’s demographics, which may differ from other geographical regions. Community pharmacy data were limited to those pharmacies participating in the sharing of fill and claims data. The cost of prescriptions was not compared between dispensing sites. The rate of prescription abandonment did not account for prescriptions purchased over the counter. The occurrence of additional acute care visits was limited to those within the health system. Further surveying of patient-specific factors in selecting a dispensing site will provide further insight for UC stakeholders. Replication of this project on a larger or continued scale would be helpful in confirming these findings
CONCLUSION
The results of the study support the use of automated drug dispensers in the UC setting to reduce the rate of prescription abandonment. The availability of point-of-care dispensing decreases the time from UC discharge to prescription pick-up and increases the likelihood for same-day prescription pick up. These findings also supported the position that the availability of automated drug dispensers can lead to lower readmission rates.
Studies such as ours improve outcomes by promoting patient-centered care and providing evidence-based data to further guide UC service lines. Adopting the use of an automated drug dispenser requires ongoing evaluation of its formulary and implementation by stakeholders of the UC team.
References
- Shrank WH, Choudhry NK, Fischer MA, et al. The epidemiology of prescriptions abandoned at the pharmacy. Ann Intern Med. 2010;153:633–640.
- Gaborcik J, Groves B, Clark A, et al. An ambulatory care clinic and community pharmacy collaboration to address prescription abandonment. Innov Pharm. 2019;10(1):1-8.
- Esposito D, Schone E, Williams T, et al. Prevalence of unclaimed prescriptions at military pharmacies. J Manag Care Pharm. 2008. 14:541-52.
- Gadkari AS, McHorney CA. Medication nonfulfillment rates and reasons: narrative systematic review. Curr Med Res Opin. 2010 Mar;26(3):683-705.
- Klein D. Medication non-adherence: a common and costly problem. Available at: https://www.panfoundation.org/medication-non-adherence/. Accessed March 7, 2023.
- Farris B, Shakowski C, Mueller S, et al. Patient nonadherence to filling discharge medication prescriptions from the emergency department: barriers and clinical implications. Am J Health Syst Pharm. 2018;75(5):316-320.
- Ginde A, von Harz B, Turnbow D, Lewis L. The effect of ED prescription dispensing on patient compliance. Am J Emerg Med. 2003;21(4):313-315.
- Weiss A, Jiang H. Overview of clinical conditions with frequent and costly hospital readmissions by payer, 2018. Hcup-us.ahrq.gov. Available at: https://www.hcup-us.ahrq.gov/reports/statbriefs/sb278-Conditions-Frequent-Readmissions-By-Payer2018.jsp#:~:text=The%20overall%20readmission%20rate%20was%2014.0%20per%20100,charge%20stays%20to%20%2416%2C400%20for%20privately%20insured%20stays. Published 2021.
Manuscript submitted November 9, 2022; accepted January 17, 2023.
Author affiliations: Emilie M. Collongette, PharmD, BCMTMS, Baptist Health South Florida Clinical Pharmacy Enterprise. Sara Panella, PharmD, BCPS, Baptist Health South Florida Clinical Pharmacy Enterprise. Michael A. DeCoske, PharmD, BCPS, Baptist Health South Florida Clinical Pharmacy Enterprise. Ernesto Sanz Martinez, MD, Affiliation Pending.