Published on
Patrick O’Malley, MD
Urgent Message: Clinicians can apply best-practice care principles for lacerations of the hand in the urgent care setting by gaining a better understanding of the anatomy and wound repair techniques. Such competency can also help reduce non-indicated referrals to the emergency department.
Citation: O’Malley P. Does This Finger Laceration Need Immediate Vascular Surgery Consultation Perspectives Based on an Urgent Care Patient Experience. J Urgent Care Med. 2024;18(4): 28-30
Key words: laceration, finger injury, suturing, urgent care
Lacerations are a common presenting complaint to urgent care (UC) clinics. Unfortunately, many UC clinicians have limited experience and confidence with suturing and laceration management. Better understanding of anatomy and basic wound care principles is important for increasing UC clinician confidence and minimizing non-indicated referrals to higher levels of care.
Introduction
Acuity degradation is an increasingly recognized issue facing urgent care in America. Acuity degradation refers to the trend demonstrating lower average complexity of presentations in UC centers. One manifestation of this phenomenon is that UC clinics are caring for fewer lacerations than in previous decades. The reasons for acuity degradation are multifactorial and synergistic with one another.1
This case presentation illustrates how provider deficiencies in understanding of the anatomy of the hand and inadequate confidence in basic wound management resulted in a patient being referred to the emergency department (ED) for a 1.5 cm laceration of the finger. (Figure 1)

Case Presentation
The patient presented to urgent care shortly after accidentally lacerating her finger with a pair of scissors. She had continued oozing, but she did not experience arterial pulsations.
Therapeutic Intervention
At the UC center, she received a tetanus vaccination, and the wound was bandaged. She was then sent to the local ED due to concern of a potentially severed artery and recommendation that she should see a vascular surgeon.


Upon arrival to the ED, there was no active bleeding. The ED clinician performed a transthecal digital block to provide anesthesia.2 The wound was irrigated with tap water at the sink, and a finger tourniquet was applied, allowing for inspection and evaluation of the wound (Figure 2).3 Four simple interrupted nylon sutures were placed (Figure 3). There was a small amount of oozing after the tourniquet was removed. Bacitracin ointment and a bandage were applied, and the patient was discharged with routine wound care and suture removal guidance.
Ethics Statement
The patient provided verbal and written consent for case description and clinical images to be used for education purposes.
Discussion
Management of lacerations requires a fundamental knowledge of relevant regional anatomy, principles of acute wound care, and the technical skills necessary for wound repair. However, it is understandable that providers with limited exposure to laceration care may be overwhelmed in such scenarios. The expectation of some bleeding and tissue distortion is crucial to avoid panic in the urgent care setting and reflexive ED referrals.
A better understanding of finger anatomy (Figures 4-5) may have mitigated this patient’s unnecessary referral. Her wound was not near any major artery—as the digital arteries are deeper and more lateral.
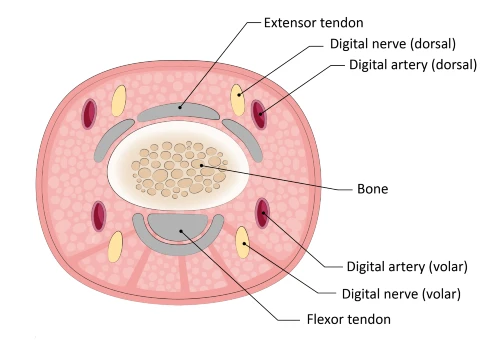
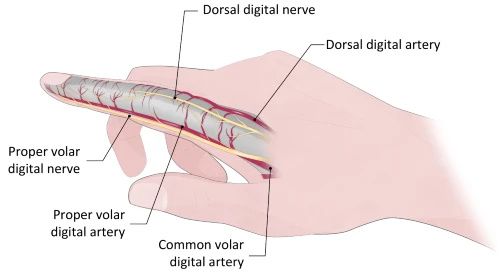
There is significant collateral and redundant circulation in the finger. Even if one of the small dorsal or volar arteries are injured, orthopedic or vascular surgery is not required unless there are signs of ischemia.4 Wound closure would be the primary treatment and is useful for achieving hemostasis.
This case demonstrates how the knowledge of relevant anatomy and the principles of acute wound care are perhaps more important than technical suturing skills in appropriate care for lacerations. The four interrupted sutures ultimately used for wound closure were simple as a repair technique, however, having the necessary knowledge of the anatomy, physiology, pharmacology, and applying it appropriately for a simple repair was equally requisite.
Additionally, hand injuries can result in important loss of function and subsequently disability, so it is critical for UC clinicians to be familiar with indications for immediate ED referral. These include:4,5
- High-pressure injection injury
- Open fracture/dislocation with bone protrusion or gross contamination
- Concerns for severe infection (eg, flexor tenosynovitis, necrotizing soft tissue infection)
- Animal or human bite wound with evidence of deep tissue involvement or infection
- Concerns for acute digital ischemia
- Partial amputation with visible bone or complete amputation
If immediate clinic or phone consultation with a hand specialist is available, this is reasonable (and often preferable as an alternative). Importantly, tendon injuries are commonly repaired in a somewhat delayed fashion, and ED referral can be deferred if follow-up with an orthopedist within 24-48 hours can be assured.6 In such cases, irrigation, loose skin approximation, and splinting in UC is a reasonable practice.
Patient Perspective
The patient presented in this case had an unfavorable opinion about her urgent care experience. From her perspective, she expected this small wound could be fully addressed in the UC center. Instead, she incurred significant additional hassle, wait time, and financial costs as a result of following the guidance of the UC provider.
Conclusion
While acuity degradation is an ongoing phenomenon in urgent care in the United States, patients with lacerations still present to UC centers frequently. UC clinicians can improve patient experience and mitigate excessive ED referrals by ensuring adequate understanding of relevant anatomy and wound care closure techniques and principles.
Manuscript submitted May 1, 2023; accepted November 29, 2023.
Author Affiliation: Patrick O’Malley, MD, Emergency Medicine, Newberry County Memorial Hospital. Author has disclosed a relevant financial interest in Medline Industries in the form of consulting and product/royalty licensing fees.
References
- Barlow B, Ayers A, Sadler, M. How Urgent Care Can Address Its Degrading Scope of Practice. November 30, 2022. Accessed June 12, 2023. https://www.jucm.com/how-urgent-care-can-address-its-degrading-scope-of-practice/
- Morrison WG. Transthecal digital block. Arch Emerg Med. 1993;10(1):35-38. doi:10.1136/emj.10.1.35.
- O’Malley, PM. Essential Tools for Urgent Care-Finger Tourniquet. June 30, 2022. Accessed June 12, 2022. https://www.jucm.com/essential-tools-for-urgent-carefinger-tourniquet/
- Luczak BP, Maher R, Gurfinkel R, Teh LG. Closed digital artery injury. Ochsner J. 2011 Summer;11(2):139-42. PMID: 21734853; PMCID: PMC3119218.
- Hunt TJ, Powlan FJ, Renfro KN, et al. Common Finger Injuries: Treatment Guidelines for Emergency and Primary Care Providers [published online ahead of print, 2023 Feb 3]. Mil Med. 2023;usad022. doi:10.1093/milmed/usad022
- Vasdeki D, Varitimidis SE, Chryssanthakis C, Stefanou N, Dailiana ZH. Medicolegal risks associated to hand and wrist trauma. World J Crit Care Med. 2022 Jan 9;11(1):40-47. doi: 10.5492/wjccm.v11.i1.40. PMID: 35433308; PMCID: PMC878 8205.
- Venkatramani H, Varadharajan V, Bhardwaj P, Vallurupalli A, Sabapathy SR. Flexor tendon injuries. J Clin Orthop Trauma. 2019 Sep-Oct;10(5):853-861. doi:10.1016/j.jcot.2019.08.005. Epub 2019 Aug 19. PMID: 31528057; PMCID:PMC6739511.
Download the article PDF: Does This Finger Laceration Need Immediate Vascular Surgery Consultation? Perspectives Based on an Urgent Care Patient Experience
