Published on
Urgent message: Cutaneous abscesses are common presentations in urgent care. While either methicillin-sensitive or methicillin-resistant Staphylococcus aureus accounts for up to 75% of skin abscesses, atypical organisms such as nontuberculous mycobacteria (NTMB) can also lead to abscess formation. Urgent care providers should be aware that the clinical presentation may be atypical and require specialized treatment.
Rachel Hughes, MD and Erik Butler, DO
CASE PRESENTATION
A 26-year-old female with no known past medical history other than depression presented to urgent care with a complaint of a nonhealing sore on her thigh for 2 months. She was most concerned for a possible spider bite. A red sore had been present on her right thigh for 2 months, but in the preceding 2 days had become bigger and more tender. She denied systemic symptoms or drainage from the lesion. She denied a history of recurrent abscesses, methicillin-resistant Staphylococcus aureus (MRSA), IV drug use, new tattoos or piercings, recent travel, or known insect bites. She worked as an administrator in a tattoo parlor but did not handle tattoo equipment. On exam, patient was afebrile and well-appearing with normal blood pressure and pulse rate. She had multiple, well-healed facial piercings and body tattoos. On her right thigh was a 2×2 cm oval purplish macule in raised indurated edges. There was spongy fluctuance in the center of the lesion with a small area of central erosion. (Figure 1.)

Figure 1. The satellite erythematous papules on the right thigh appeared after adhesive bandaging. The patient reported this was a typical reaction to adhesive.
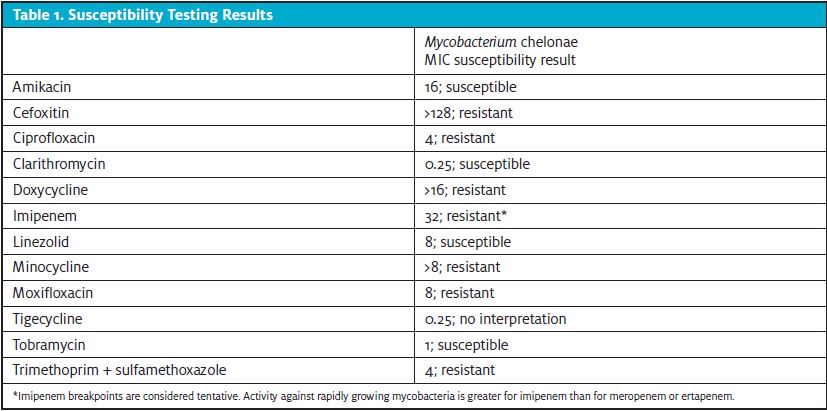
An incision-and-drainage (I&D) procedure performed with a 3 mm punch blade revealed a minimal amount of sanguine-purulent fluid from an empty wound cavity. Differential diagnosis at the time included simple cutaneous abscess, folliculitis, insect bite/sting with necrosis, infected abrasion or skin trauma, or infected epidermal inclusion cyst. The most likely pathogen was thought to be Staphylococcus or Streptococcus species, given the typical prevalence of these organisms in skin infections. However, a gram stain and culture were obtained given the indolent course and atypical appearance of the lesion. Patient was given local wound care instructions and prescribed doxycycline 100 mg daily twice daily for 7 days to cover for methicillin-sensitive S aureus and MRSA. Gram stain initially resulted with 2+ WBCs and no organisms seen. However, preliminary culture results on the same day revealed rapidly growing Mycobacterium. Fourteen days after the preliminary culture, Mycobacterium chelonae was reported along with sensitivity results. (Table 1.)
The patient was referred to Infectious Disease for consult, given the atypical organism identified and case reports of complicated antibiotic regimens required to effectively treat mycobacterial skin infections.
Further history revealed the patient did have a history of IV drug use with recent relapse (though this occurred after the abscess appearance), as well as chronic untreated hepatitis C. She also revealed that she was shaving her legs in an outdoor hot tub prior to developing the skin lesion. She continued to deny systemic symptoms including fever, chills, fatigue, respiratory symptoms, or weight loss that would indicate progression or dissemination of M chelonae infection. On exam, the infection remained localized to the soft tissue of her right though without significant progression of healing.
Treatment, Outcome, and Follow-Up
Given the localized nature of infection, the patient was treated with linezolid 600 mg daily and clarithromycin 500 mg twice per day for 4-6 months, pending clinical improvement. Baseline CBC and CMP were checked for linezolid monitoring.
DISCUSSION
M chelonae is a non-motile, non-spore-forming, gram-positive, acid-fast bacillus. It is classified as a rapidly growing NTMB, class IV in the Runyon classification. Cases of infection have been reported globally with no seasonal trend or association with a specific sex, race, or age group. Pertinent to our case, M chelonae has been shown to be resistant to chlorine and identified in water systems, though typically grows at lower temperatures (30°-32°C).1
M chelonae infections present most often as a pustule, hemorrhagic crust, or abscess in areas of puncture wounds or skin trauma, often on the extremities. It has been reported after tattoos, acupuncture, sclerotherapy, injectable medication, and other injection procedures. The eye is the second most frequent site of infection. Disseminated skin involvement and invasive infections (such as infection of bone, joint, or muscle) can occur in immunocompromised patients. Pulmonary infection is rare but patients with cystic fibrosis can be colonized with M chelonae.1,2
Treatment of M chelonae and NTM can be challenging. Expert consultation and sensitivities should be pursued given the potential for resistance patterns, multidrug regimens, and need for prolonged antibiotic treatment durations. The American Thoracic Society and Infectious Diseases Society of America recommend an oral macrolide initially (for example, clarithromycin monotherapy) combined with cefoxitin, amikacin, or imipenem-cilastatin for the treatment of cutaneous infections.3 Combination therapy with at least two agents is recommended due to potential development of resistance during prolonged therapy.3 For treatment of disseminated or invasive disease, 4-6 months of systemic therapy is recommended. Other treatment modalities include local antiseptic and antibacterial therapy, repetitive surgical debridement, and I&D of abscesses.3
As with our patient, abscesses that do not respond to initial I&D may require further surgical excision or debridement.
The prevalence of M chelonae and rapidly growing NTM infections is increasing but they remain a rare cause of skin and soft-tissue infections.
NTM skin infections should be considered in the differential for abscesses with an atypical appearance, in infections that do not responsive to initial standard treatment, or if patient presents with skin infection after an invasive procedure. Current IDSA guidelines recommend gram stain and culture of pus from carbuncles and abscesses, but treatment is also reasonable without culture in typical cases. In addition, I&D is the recommended treatment for abscesses (as opposed to antibiotics alone). Antibiotics against S aureus can be used as an adjunct to I&D, especially if the patient has features concerning for systemic inflammatory response syndrome (SIRS). An antibiotic against MRSA is recommended in patients who have failed initial antibiotic treatment, are immunocompromised, or in patients with SIRS and hypotension.4
This case highlights the importance of considering gram stain and culture during abscess I&D or before treatment of purulent cellulitis. If initial culture is unrevealing or infection is not responding to typical coverage for gram-positive organisms, then biopsy or acid-fast staining should be considered.
TAKE-HOME POINTS
- Consider gram stain and culture during abscess I&D or before treatment of purulent cellulitis.
- Consider NTM skin infections with abscesses with atypical appearance, indolent course, or not responsive to typical therapy.
- Obtaining sensitivities is important for appropriate treatment of NTM skin and soft tissue infections given resistance patterns.
REFERENCES
- Akram SM, Rathish B, Saleh D. Mycobacterium chelonae. Updated January 31, 2021. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; January 2021. Available at: https://www.ncbi.nlm.nih.gov/books/NBK430806/. Accessed November 10, 2021.
- 2. Misch EA, Saddler C, Davis JM. Skin and soft tissue infections due to nontuberculous mycobacteria. Curr Infect Dis Rep. 2018;20(6) Available at: https://doi.org/10.1007/s11908-018-0611-3. Accessed November 10, 2021.
- Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367-416. Erratum in: Am J Respir Crit Care Med. 2007 Apr 1;175(7):744-745. Dosage error in article text.
- Stevens DL, Bisno AL, Chambers HF, et al. Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2014;59(2):e10–e52.
- Wentworth AB, Drage LA, Wengenack NL, et al. Increased incidence of cutaneous nontuberculous mycobacterial infection, 1980 to 2009: a population-based study. Mayo Clin Proc. 2013;88(1):38-45.
- Cassidy PM, Hedberg K, Saulson A, et al. Nontuberculous mycobacterial disease prevalence and risk factors: a changing epidemiology. Clin Infect Dis. 2009;49(12):e124–e129.
- Smith GS, Ghio AJ, Stout JE, et al. Epidemiology of nontuberculous mycobacteria isolations among central North Carolina residents, 2006–2010. J Infect. 2016;72(6):678–686.
Author affiliations: Rachel Hughes, MD, University of North Carolina School of Medicine Department of Family Medicine. Erik Butler, DO, University of North Carolina School of Medicine Department of Family Medicine. The authors have no relevant financial relationships with any commercial interests.
View More Articles on Abscesses
- Actinomyces Neuii As A Cause Of Vulvar Abscess
- CA-MRSA Abscess Care And Treatment Guidelines In Urgent Care Practice
- Practice Review: Patients Presenting With Symptoms Of Odontogenic Infection