Published on
Urgent message: Acute otitis media (AOM) is the leading diagnosis for antibiotic prescribing in pediatric patients. As antibiotic stewardship becomes more essential in preventing antibiotic resistance, safe and effective management of AOM becomes all the more important in urgent care. The treatment path should reflect nuances in management to inform decisions regarding the necessity of antibiotics—and if they are deemed necessary, targeting the type, delivery vehicle, and duration to keep a narrow treatment effect.
When should I suggest ‘watchful waiting’?
Consider watchful waiting, rather than immediate antibiotic treatment, for patients older than 6 months of age with unilateral AOM, mild otalgia, and temperature less than 39˚C or for children older than 2 years of age with unilateral or bilateral AOM without otorrhea and only mild symptoms.1 High fever, severe pain, ill appearance, or symptom duration greater than 48 hours are generally situations in which watchful waiting is not recommended, regardless of age. Patients who meet criteria for watchful waiting can be discharged without antibiotics if they have adequate follow-up should symptoms worsen. An alternative option is to offer the family a safety net antibiotic prescription and instruct the family to fill the prescription in 2-3 days only if the child does not improve.1
What antibiotics should I consider for uncomplicated AOM?
The first-line therapy for routine AOM is typically amoxicillin (80-95 mg/kg/day divided bid). The duration of therapy in children less than 2 years of age should be 10 days, while shorter courses can be considered in older children. The clinician should consider alternate initial therapy if the patient has high risk of S pneumoniae resistance, a recent episode of AOM (within 30 days), a penicillin allergy, or concomitant bacterial conjunctivitis.1
When should I consider treatment failure, and what are my options?
Clinical improvement of AOM is expected within 2-3 days. If the patient is not improving in this timeframe, the clinician should consider changing to a secondary antibiotic. It is difficult to consider antibiotic failure until the patient has received at least four or five doses of an appropriately dosed twice-daily oral antibiotic (eg, amoxicillin, amoxicillin-clavulanate) or two or three doses of an appropriately dosed once-daily oral antibiotic (eg, azithromycin, cefdinir).
Secondary antibiotic regimens include amoxicillin-clavulanate or cefdinir. Tertiary antibiotic regimens could include either intramuscular ceftriaxone or combination oral therapy with clindamycin and trimethoprim-sulfamethoxazole (TMP-SMX).1 For patients with inability to tolerate oral antibiotics or with perceived antibiotic failure, intramuscular ceftriaxone (50 mg/kg q 24 hrs for 2-3 days) is preferred. If the patient’s AOM does not resolve with intramuscular ceftriaxone, referral to otolaryngology is recommended to consider tympanocentesis or myringotomy to identify the causative organism.1
How should I respond to the question, Does my child need tympanostomy tubes (TTs)?
For most children, tympanostomy tubes are generally considered in the first 3 years of life when frequent upper respiratory infections lead to recurrent AOM. The definition of recurrent AOM is ≥3 episodes in 6 months, or ≥4 in 12 months with the most recent episode in the preceding 6 months.2 It is therefore important to make an accurate diagnosis of AOM since recurrent episodes may lead to surgical therapy. Recurrent AOM in older children is similarly caused by eustachian tube dysfunction but more often requires adenoidectomy in addition to TT placement. If a child presents with recurrent AOM, providers can discuss the possibility of tympanostomy tubes with families and advise them to speak to their primary care provider about a possible otolaryngology referral. In order to preserve patients’ relationships with the medical home, urgent care providers should only refer children directly to an otolaryngologist in unusual circumstances.2
If a patient has patent TTs, how does the treatment of AOM differ?
Patients with patent tympanostomy tubes may routinely have otorrhea as a sign of middle ear disease, often without pain or fever, especially in the setting of an upper respiratory infection. Acute otorrhea resolves on its own without treatment in half of patients, especially if the tubes are widely patent; however, it is generally recommended to treat acute otorrhea with topical antibiotics with or without steroids. Special attention should be made to choose ear drops safe for use with a patent middle ear. Fluoroquinolones are the only FDA-approved topical therapies for children with a non-intact TM. Aminoglycoside (gentamicin) and polymyxin drops are considered ototoxic and are contraindicated.3 Topical steroids may improve the efficacy of the antibiotic but are often more expensive and make the drops more viscous and leave residue in the ear canal. Addition of an oral antibiotic is generally not indicated for acute otorrhea but should be considered if the patient has a high fever, ill appearance, severe ear pain, is immunocompromised, or has significant concurrent illness (eg, sinusitis, pneumonia, etc.). Using oral antibiotics does not discount the need for topical therapy. Compared with oral amoxicillin-clavulanate, topical fluoroquinolones have better coverage against P aeruginosa, which is a common pathogen in older children with TTs and otorrhea.4 If topical antibiotics are required for more than 7 days, consider initiating an oral antibiotic or refer to the patient’s otolaryngologist. Children with patent TTs should avoid getting water in their ears while being treated for otorrhea and should not use over-the-counter eardrops that are unsafe for middle ear patency.4
What if I can’t tell if the TTs are patent and intact?
Most children have short-term (grommet) tubes which typically last about 12 months (range of 4-18 months). Some children with craniofacial abnormalities receive long-term (T-tubes) that have anchors to stay in longer than 15 months.4 Grommet tubes are unlikely to still be functional after 12-18 months, so incomplete visualization in this age group should be assumed to have nonfunctional or extruded TTs.
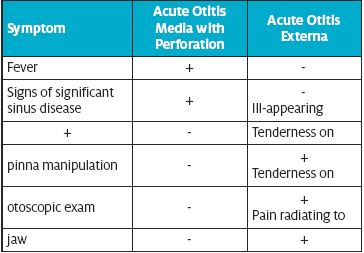
How do I differentiate perforated AOM from acute otitis externa (AOE)?
Since both conditions may present with otorrhea and otalgia, it can be difficult to distinguish these diagnoses on examination without being able to visualize the TM. Generally, AOE is not associated with fever, and children with AOE do not appear ill.3 Patients with AOE may have severe pain with positioning of the pinna to insert the ear speculum, as well as exquisite tenderness when the ear speculum is inserted into the ear canal. Patients with AOM with perforation in contrast generally do not have severe ear canal sensitivity or pain with manipulation of the pinna. Making an accurate diagnosis is important because the treatment paths are different for AOE and AOM with perforation. AOE is treated with topical antibiotics (with or without corticosteroids) alone, whereas AOM with perforation should be treated with oral antibiotics (with or without topical therapy).
PITFALLS
Don’t miss mastoiditis
Mastoiditis is the most common complication of AOM. Mastoiditis with osteitis/periosteal abscess typically needs surgical intervention. Signs and symptoms of mastoiditis include swelling and erythema around the ear, mastoid bone tenderness, loss of the postauricular crease, and anterior and inferior displacement of the pinna.2 Patients are often ill-appearing, and this needs to be distinguished from a periauricular cellulitis. It is helpful to examine the postauricular area and external ear, especially when the patient is febrile or has recurrent or chronic AOM.2
Don’t assume penicillin allergy requires alternate therapy
Patients frequently report penicillin allergy, forcing some clinicians to use macrolide therapy as an alternative. Macrolide therapy (eg, azithromycin), however, is often inadequate AOM treatment because of poor efficacy against S pneumoniae and H influenzae. Similarly, S pneumoniae has shown increasing resistance to trimethoprim-sulfamethoxazole (TMP-SMX).1 It’s important to ask more questions when patients report penicillin allergy. As many as 90% of patients who self-report a penicillin allergy do not exhibit IgE-mediated sensitization to penicillin.5 In the absence of acute allergic reaction characterized by urticaria or signs of anaphylaxis, third-generation cephalosporins carry a negligible risk of cross-allergy6 and should be considered.
Don’t forget to address pain control
Whether prescribing antibiotics or not, it’s important to address analgesia with the use of NSAIDs adequately dosed for a child’s weight. Families often ask if there are any eardrops to help with the pain and, unfortunately, topical analgesics do not add significant benefit. For this reason, in 2015 the FDA unapproved otic drops marketed as analgesics containing benzocaine, antipyrine, and pramoxine. Other natural treatments of pain, like topical application of heat or cold to the ear or using oils in the ear, are not well studied and have limited effectiveness. Using oils or drops not prescribed by a provider can be dangerous in the setting of a perforated tympanic membrane.
SUMMARY
AOM is a common diagnosis in urgent care, and appropriate management can come with many obstacles ranging from treatment failure to questions about tympanostomy tubes. The pearls and pitfalls addressed in this article can aid in the evaluation and management of AOM and complications, to arm clinicians with strategies to improve antibiotic stewardship in AOM treatment. Recommended additional resources include American Academy of Pediatrics clinical practice guidelines on the diagnosis and management of acute otitis media and the American Academy of Otolaryngology–Head and Neck Surgery’s clinical practice guideline on tympanostomy tubes in children.
Citations
- Lieberthal A, Carroll A, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013;131(3):964-999.
- Schilder A, Rosenfeld R, Venekamp R. Acute otitis media and otitis media with effusion. In: Flint P, Francis H, Haughey M, et al, eds. Cummings Otolaryngology: Head and Neck Surgery. Philadelphia, PA: Elsevier Inc.;2021: 2956-2969.
- Haddad J, Dodhia S. External otitis. In: Kliegman R, St. Geme III J, Blum N, et al, eds. Nelson Textbook of Pediatrics. Philadelphia, PA: Elsevier Inc.: 3414-3417
- Rosenfeld RM, Schwartz SR, Pynnonen MA, et al. Clinical practice guideline: tympanostomy tubes in children. Otolaryngology Head Neck Surg. 2013;149(1 Suppl):S1-S35.
- Raja AS, Lindsell CJ, Bernstein JA, et al. The use of penicillin skin testing to assess the prevalence of penicillin allergy in an emergency department setting. Ann Emerg Med. 2009;54(1):72.
- Campagna JD, Bond MC, Schabelman E, et al. The use of penicillin-allergic patients: a literature review. J Emerg Med. 2012:42(5):612-620
Kathryn Doran, DO, FAAP is a pediatrician at Children’s Mercy Kansas City; a Clinical Assistant Professor of Pediatrics at the University of Missouri-Kansas City School of Medicine; and a Clinical Assistant Professor of Pediatrics at the University of Kansas School of Medicine.