Published on
Download the article PDF: An Evaluation Of Unnecessary Prophylactic Antibiotics For Clean Lacerations
Urgent Message: Prophylactic antibiotic prescribing for patients with clean lacerations is a common but unnecessary practice. Rates of prescribing did not differ based on type of provider or physician specialty in this study of 20 urgent care centers.
Michael Smart, PhD; Jennifer Bush, MSN, APRN, FNP-C/ENP-C
Keywords: antimicrobial stewardship; prophylactic antibiotics; laceration repair; urgent care
Abstract
Background: Oral prophylactic antibiotics for clean lacerations that require suture repair are commonly prescribed when they are unneeded. We aimed to evaluate the frequency of this practice in the urgent care setting.
Methods: This retrospective cross-sectional study used electronic health record data from 20 urgent care centers within an institutional healthcare system in the Southeast. The frequency of antibiotic prescribing was assessed for patients who presented with a clean laceration requiring suture repair. A subanalysis evaluated differences in prescribing patterns between physicians and advanced practice providers (APPs), as well as physicians by specialty.
Results: Approximately 56% of patients with clean lacerations that had suture repair were prescribed prophylactic antibiotics (n=182/323). Practices did not differ between physicians or APPs (p=0.79), nor among physicians by specialty (p=0.17). Prophylactic antibiotics were prescribed for a mean duration of 7 ±1.82 days. Antibiotics were more likely to be prescribed when more sutures were placed.
Conclusion: Prophylactic antibiotic prescribing for patients with clean lacerations is a common but unnecessary practice. Rates of prescribing did not differ based on type of provider or physician specialty in the urgent care setting.
Introduction
Clean lacerations requiring suture repair are frequently encountered in the urgent care setting. While suturing these wounds is often a straightforward clinical skill, the decision of whether or not to prescribe prophylactic antibiotics to prevent infection can present a clinical dilemma. A clean laceration is defined as one occurring from a clean object, not resulting from a puncture or bite, and is without dirt, soil, feces, or saliva.[1],[2] They are considered low risk for infection.[3]
Despite this low risk, many providers choose to prescribe antibiotics unnecessarily for these wounds. Prophylactic antibiotics have not been found to reduce the rates of infection for clean hand lacerations regardless of patient age, comorbid diabetes, or closure technique.3,[4],[5],[6] When prophylactic antibiotics are prescribed, recommendations include that they are given for the shortest duration possible, as longer courses confer no additional benefit and are associated with antimicrobial resistance and antibiotic-associated adverse events.[7],[8]
Reducing inappropriate antibiotic prescribing for simple, clean lacerations represents an important avenue to decrease unnecessary antibiotic prescribing and ultimately reduce the risk of developing antimicrobial resistance, a public health crisis. While traditional research and quality improvement interventions have focused on inappropriate antibiotic prescribing for infections, including viral upper respiratory infections,[9],[10] urgent care settings provide a unique opportunity to reduce antibiotic use in other conditions, including those for clean lacerations.
Although existing evidence does not support the use of prophylactic antibiotics for clean lacerations, limited data exist regarding how frequently this evidence is adhered to in urgent care settings. Additionally, there is a paucity of data examining the length of prophylactic antibiotic prescribing in the outpatient setting. Therefore, we aimed to understand the prevalence and duration of prescribed prophylactic antibiotics for clean lacerations repaired with sutures.
Methods
This study examined electronic healthcare record (EHR) data from a network of 20 urgent care centers embedded within a large, metro-Atlanta healthcare system. This practice is unique in that it sees a large volume of patients—more than 300,000 annually—and employs approximately 75 providers with a variety of training backgrounds including both physicians with training in emergency medicine, family medicine, and internal medicine/pediatrics, as well as advanced practice providers (APPs) (nurse practitioners [NP] and physician assistants [PA]).
Selection and Description of Participants
This study used a retrospective, cross-sectional chart review method and included 3 months of data from January 2023 through March 2023. Cases that required lacerations were identified using procedure codes for laceration repair. Encounters that documented the use of glue, staples, wound closure strips, or other types of closures were excluded. Additional exclusion criteria included patients who had a documented history of human immunodeficiency virus, were undergoing chemotherapy, receiving immunomodulating or immunosuppressing medications, had a history of diabetes, had a documented contaminated wound, were under the age of 18 years, or 85 years or older. Excluded cases were identified by both evaluating patient diagnoses listed in the medical chart as well as medications. The decision to exclude these individuals was informed by the lack of literature that evaluated the effectiveness of prophylactic antibiotics in these populations as well as their potentially higher susceptibility to bacterial infections and likewise possible benefit from prophylactic antibiotics.
Data related to prescribed oral antibiotics were extracted from patient encounters. The study identified an oral prophylactic antibiotic as an oral antibiotic that was prescribed and had a start date on the same day of the patient encounter. Topical antibiotics, such as topical bacitracin or mupirocin, were not considered in the analysis.
Data quality was ensured through a manual chart review of 5% of cases by the study authors. Institutional review board approval was waived by the organization given the nature of the study.
Statistics
Descriptive statistics were used to evaluate the average number of sutures placed, location of lacerations, name of antibiotic prescribed, and duration of antibiotic treatment.
A chi-square test was used to evaluate differences in the frequency of prophylactic antibiotics prescribed by the level of the training of the prescriber (DO, MD, NP, PA). An analysis in the physician subgroup evaluated whether prescribing practices differed based on physician specialty (emergency medicine, family medicine, internal medicine/pediatrics). A Mann-Whitney test was used to examine the difference in the number of sutures placed between the group that had a prophylactic antibiotic prescribed and the group that did not.
Statistical analysis was completed using SPSS (Version 29). An alpha level of <0.05 was used to determine statistical significance.
Results
In the urgent care system, a total of 462 lacerations were repaired with sutures during the 3-month period. After application of the exclusion criteria, a total of 323 patient encounters were included in the final analysis.
The average number of simple sutures placed per encounter was 5.1 (range 1-19). The hand was the most common location for suture repair (n=180), followed by the head/neck (n=55). Overall, 56% of patients who received suture repair for a laceration received antibiotics (n=182).
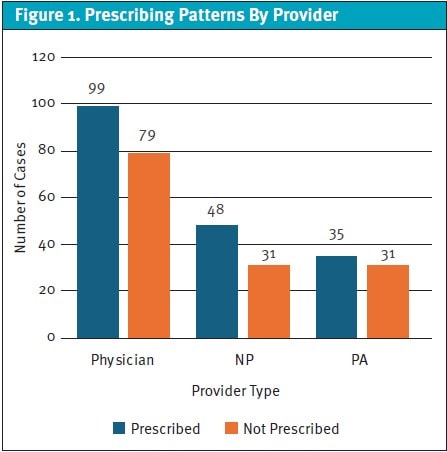
There was no difference in the frequency of prophylactic antibiotic prescribed between MDs, DOs, PAs, or NPs (χ²(1, N=323) =1.04, p=0.79) (Figure 1). There was no difference in prescribing patterns for prophylactic antibiotic when the specialty of physicians was considered (emergency, family, internal medicine/pediatrics) (χ²(1, N=178) =3.51, p=0.17). A Mann–Whitney test revealed a difference in the number of sutures placed between the group prescribed a prophylactic antibiotic (median 5, interquartile range 3–7) and the group that was not (median 4, interquartile range 3–5) (U=10,414.50, z= –2.14, p=0.032, r=0.12).
For patients who received a prophylactic antibiotic, the average length of treatment was 7.0 days ±1.82 days. The most common antibiotic prescribed was cephalexin (n=118). Other antibiotics included amoxicillin-clavulanate (n=29), trimethoprim-sulfamethoxazole (n=14), doxycycline (n=10), amoxicillin (n=7), doxycycline/metronidazole (n=2), cefdinir (n=1), and clindamycin (n=1).
Discussion
This study highlights the high proportion of patients with clean lacerations that inappropriately receive antibiotics. Given the increased incidence of antimicrobial resistance, limiting prophylactic antibiotic use in these encounters represents an important avenue for antimicrobial stewardship programs.
Additionally, there was a significant variation in both the type of prophylactic antibiotic that was prescribed and the length of antibiotic prescribing. The average duration of antibiotics was 7 days, well beyond the traditional 3-5 days duration of antibiotics that should be used when prescribed prophylactically.7 Although considered unnecessary in most cases, prescribed prophylactic antibiotics should be given for the minimum duration necessary to reduce antimicrobial resistance.
This study found that this practice of prescribing prophylactic antibiotics did not differ between type of provider and likewise did not differ in a subanalysis of physician specialty types. This may highlight the lack of training and education that providers, both physicians and APPs, receive regarding suture repair care and when prophylactic antibiotics are indicated. There may be other factors such as patient expectations that also contribute to this practice of prescribing prophylactic antibiotics.
Future studies should focus on why providers make decisions to prescribe antibiotics for clean lacerations requiring suture repair and likewise develop interventions to improve provider knowledge related to this type of prescribing.
Limitations
There are several limitations to this study that may limit the generalizability of the findings. First, this study limited analysis to prophylactic antibiotic prescribing in 1 location in the country. Prescribing practices may vary in other institutions and geographic regions. Additionally, this study analyzed information from coded data and did not include text analysis from typed notes. This may have omitted manually typed information from providers on their decision-making processes in prescribing prophylactic antibiotics.
Conclusion
Prophylactic antibiotic prescribing for clean lacerations requiring suture repair is a common, often unnecessary practice in urgent care. Future investigations should evaluate why providers make decisions to prescribe prophylactic antibiotics and evaluate interventions to reduce this inappropriate prescribing.
This study was not funded.
The authors would like to acknowledge and thank Michelle Gaddis for her contribution to this study.
Manuscript submitted July 9, 2025; accepted December 7, 2025.
References
- [1]. Centers for Disease Control and Prevention. Clinical guidance for wound management to prevent tetanus. Published June 10, 2025. Accessed December 12, 2025. https://www.cdc.gov/tetanus/hcp/clinical-guidance/index.html
- [2]. Forsch RT, Little SH, Williams C. Laceration repair: a practical approach. Am Fam Physician. 2017;95(10):628-636.
- [3]. Roodsari GS, Zahedi F, Zehtabchi S. The risk of wound infection after simple hand laceration. World J Emerg Med. 2015;6(1):44-47. doi:10.5847/wjem.j.1920-8642.2015.01.008
- [4]. Berwald N, Khan F, Zehtabchi S. Antibiotic prophylaxis for ED patients with simple hand lacerations: a feasibility randomized controlled trial. Am J Emerg Med. 2014;32(7):768-771. doi:10.1016/j.ajem.2014.03.043
- [5]. Cummings P, Del Beccaro MA. Antibiotics to prevent infection of simple wounds: a meta-analysis of randomized studies. Am J Emerg Med. 1995;13(4):396-400. doi:10.1016/0735-6757(95)90122-1
- [6]. Reeder TJ, Thomas SH, Fitch MT, et al. Evaluating and preparing wounds. In: Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM, eds. Tintinalli’s Emergency Medicine Manual. 7th ed. McGraw-Hill Education; 2012:81-84.
- [7]. Appelbaum RD, et al. Antibiotic Prophylaxis in Injury: An American Association for the Surgery of Trauma Critical Care Committee clinical consensus document. Trauma Surg Acute Care Open. 2024;9(1):e001304. doi:10.1136/tsaco-2023-001304
- [8]. Grant J, Saux NL; Members of the Antimicrobial Stewardship and Resistance Committee (ASRC) of the Association of Medical Microbiology and Infectious Disease (AMMI) Canada. Duration of antibiotic therapy for common infections. J Assoc Med Microbiol Infect Dis Can. 2021;6(3):181-197. doi:10.3138/jammi-2021-04-29
- [9]. Centers for Disease Control and Prevention. US Antibiotic Awareness Week partner toolkit. Published November 17, 2025. Accessed December 12, 2025. https://www.cdc.gov/antibiotic-use/php/usaaw-partner-toolkit/index.html
- [10]. Kadi B, Shawar S, Agnello S, Coe K, Delatore L, Dutton JR, Rozycki E. Integrating an antimicrobial stewardship bundle into advanced urgent care sites. Antimicrob Steward Healthc Epidemiol. 2025;5(1):e246. doi:10.1017/ash.2025.10178
Author Affiliations: Michael Smart, PhD, Western Michigan University Homer Stryker MD School of Medicine, Kalamazoo, Michigan. Jennifer Bush, MSN, APRN, FNP-C, ENP-C, Georgia State University, Atlanta, Georgia. Authors have no relevant financial relationships with any ineligible companies.