Published on
Michael Weinstock, MD; Gabby Gostigian, MD; and Matthew Delaney, MD
Urgent message: Failure to consider subtleties and the context in which a patient presents can lead to insufficient differential diagnoses and missed diagnoses that leave the patient at risk for poor outcomes and the provider at risk for litigation.
INTRODUCTION
Cellulitis from a wound infection in the urgent care is common, and so is our management: wound care and antibiotics. But consider a scenario in which a patient presents before the onset of infection and when prophylactic antibiotics need to be focused on a specific causative organism.
THE MEDICAL CASE
A 23-year-old man presented with injuries to his hands after an altercation. The patient was seen and examined with documentation of contusions and lacerations but without evidence of erythema or purulence; there was no documentation of an infection present. The patient was not prescribed antibiotics, but curiously was instructed to see an orthopedist the following morning. When the patient presented to the orthopedist the next morning, he was prescribed cephalexin for an infection, which continued to worsen. He returned to the same orthopedist 3 days later and did not have a change in management but was referred to a hand specialist. Unfortunately, the patient did not follow through with this appointment.
Closed-Fist Injuries/“Fight Bite”
The key to diagnosing and managing a closed-fist injury (CFI) is to think about the diagnosis for all lacerations over the dorsal surface of the metacarpal joints. Even in a situation where a patient offers an alternative explanation for their injury, the clinician needs to keep a high degree of suspicion.
Identification of CFIs is important, given the high risk of associated damage to deep structures due to the relatively thin skin on the dorsal surface of the knuckles; approximately 75% of cases have associated injury to underlying tendon, joint capsule, cartilage, and bone.1
Initial exam should take place after adequate pain control and hemostasis is achieved. Range-of-motion and strength testing should be performed to assess for underlying tendon injury. However, tendons with up to 80% disruption may still exhibit symmetric strength when compared with the uninjured hand.2
When examining the injury, the margins of the laceration may need to be extended to allow for better visualization of underlying structures. These structures should be examined with the interphalangeal and metacarpophalangeal joints in the flexed position because tendon injuries may be missed as they retract proximally when the hand is unclenched. In addition to a through physical exam, radiographic imaging should be obtained to assess for fractures, foreign bodies, or intraarticular air that would suggest penetration of the underlying joint.3 Any evidence or suspected damage to underlying structures warrants immediate consultation to a hand specialist.
Wound care of CFIs should be performed similarly to that of any other animal bite to the hand. CFIs should be adequately cleaned, debrided, and irrigated to optimize outcomes and prevent infections.
Irrigation is one of the mainstays for decontaminating bite wounds and is associated with up to fivefold decrease in rates of infection.4-6 Given the high rate of infection, CFIs should not be closed primarily but instead left open with a bulky dressing and splinted in a position of function.1,7-13 CFIs require reevaluation within 1-2 days of initial presentation to monitor for evidence of infection due to high rates of osteomyelitis (39%), septic arthritis (29%) and tenosynovitis (26%).7
Ideally, the patient would follow up with a hand specialist but at a minimum they should be re-evaluated so that any potential complications could be referred appropriately.
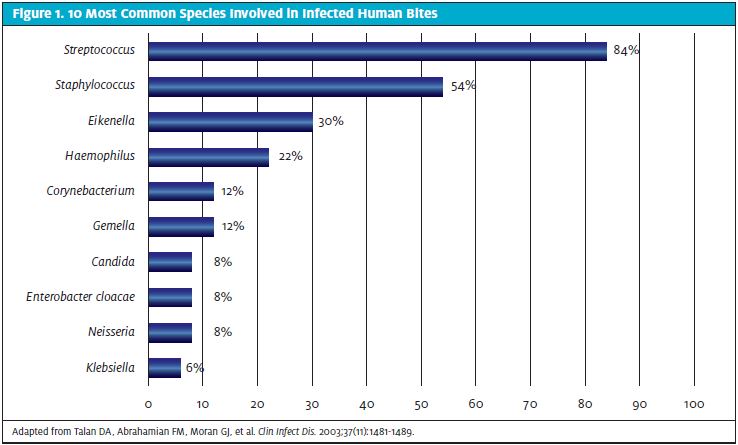
In addition to close follow-up, these patients require prophylactic antibiotics for 3-5 days.7,9-11,13-18 Infections from a CFI are often polymicrobial, with a mix of aerobic and anaerobic organisms. The most common species involved in infected human bites include Streptococcus (82%), Staphylococcus (57%), and Eikenella (30%).19 The most common prophylactic monotherapy includes amoxicillin/clavulanate or moxifloxacin.9,10,12,14-16,18,20,21 Alternative regimens include combining doxycycline, metronidazole, or clindamycin with either trimethoprim/sulfamethoxazole or ciprofloxacin.14,15,18,20,21
THE OUTCOME
When the patient did return, he had an extensive infection from his fight bite/CFI which required surgery and antibiotics. The patient was left with scarring from his little finger across the palm into the forearm. A lawsuit was filed.
THE LEGAL CASE
Allegations from the Plaintiff
Predictably, the plaintiff’s allegation was that the standard of care for a human bite wound was not met:
- Antibiotic prophylaxis needs to be directed toward causative organisms, including Eikenella corrodens, a common organism found in oral flora. This was not done.
- Follow-up was not accessible.
- Permanent scarring and loss of function would have been avoided with proper care and follow-up.
Arguments from the Defense
- The defendant was not aware that the patient’s injuries were from a human bite wound. Though they documented that they were the result of an “altercation,” it was not revealed that this altercation involved a punch to the mouth and a “closed-fist injury.”
- A culture was done at the initial examination and revealed strep, a common skin organism which did not require antibiotic prophylaxis.
- Cephalexin was the correct antibiotic for a diagnosis of cellulitis.
- The patient did not take the cephalexin as prescribed. The patient said he filled the prescription, but the pharmacy did not have a record of it being picked up).
The Legal Decision
The case proceeded to trial. A verdict was returned for the defense.
LESSONS LEARNED
How can we use this unfortunate case to improve diagnosis and management at the bedside in urgent care?
- Consider the mechanism of injury. A laceration over a knuckle is a fight bite until proven otherwise.
- When a patient has a suspected CFI, take extra steps to get an accurate history. This may include discussing potential complications, asking to speak with their friends and family, and assuring them that whatever they say will be kept confidential.22
- Document that you considered CFI for lacerations over the MCP joints even if the patient continues to deny this mechanism of injury.
- The antibiotic prophylaxis for a fight bite/CFI is different than that for normal skin infections: cover for Eikenella corrodens with amoxicillin/clavulanate.
- Even with appropriate management and timely follow-up, there may still be an adverse outcome. Ensure that the patient and family/friends are aware of this and that it is documented in the chart.
- Ensure that the patient knows the potential for progression of disease.
- Document an action and time-specific recommendations for follow-up.
REFERENCES
- Smith HR, Hartman H, Loveridge J, Gunnarsson R. Predicting serious complications and high cost of treatment of tooth-knuckle injuries: a systematic literature review. Eur J Trauma Emerg Surg. 2016;42(6):701-710.
- Henry GI. Extensor tendon lacerations. Medscape. Available at: https://emedicine.medscape.com/article/1286225-overview. Accessed September 9, 2022.
- Vijayan R, Awad G. The tooth, the whole tooth: an unusual fight bite with an unnoticed embedded tooth in the hand. BMJ Case Rep. 2015;2015:bcr2015209313.
- Callaham ML. Treatment of common dog bites: infection risk factors. JACEP. 1978;7(3):83-87.
- Goldstein EJC. Management of human and animal bite wounds. J Am Acad Dermatol. 1989;21(6):1275-1279.
- Greene SE, Fritz SA. Infectious complications of bite injuries. Infect Dis Clin North Am. 2021;35(1):219-236.
- Shoji K, Cavanaugh Z, Rodner CM. Acute fight bite. J Hand Surg Am. 2013;38(8):1612-1614.
- Bunzli WF, Wright DH, Hoang AT, et al. Current management of human bites. Pharmacotherapy. 1998;18(2):227-234.
- Patil PD, Panchabhai TS, Galwankar SC. Managing human bites. J Emerg Trauma Shock. 2009;2(3):186-190.
- Jha S, Khan WS, Siddiqui NA. Mammalian bite injuries to the hand and their management. Open Orthop J. 2014;8:194-198.
- Singer AJ, Dagum AB. Current management of acute cutaneous wounds. N Engl J Med. 2008;359(10):1037-1046.
- Brook I. Management of human and animal bite wounds: an overview. Adv Skin Wound Care. 2005;18(4):197-203.
- Henton J, Jain A. Cochrane corner: antibiotic prophylaxis for mammalian bites (Intervention review). J Hand Surg Eur Vol. 2012;37(8):804-806.
- Ball V, Younggren BN. Emergency management of difficult wounds: part I. Emerg Med Clin North Am. 2007;25(1):101-121.
- Sternberg ML, Jacobs T. Clenched fist injury. J Emerg Med. 2010;39(1):97.
- Kennedy SA, Stoll LE, Lauder AS. Human and other mammalian bite injuries of the hand: evaluation and management. J Am Acad Orthop Surg. 2015;23(1):47-57.
- Looke D, Dendle C. Bites(mammalian). BMJ Clin Evid. 2010;2010:0914.
- Moran GJ, Talan DA, Abrahamian FM. Antimicrobial prophylaxis for wounds and procedures in the emergency department. Infect Dis Clin North Am. 2008;22(1):117-143, vii.
- Talan DA, Abrahamian FM, Moran GJ, et al. Clinical presentation and bacteriologic analysis of infected human bites in patients presenting to emergency departments. Clin Infect Dis. 2003;37(11):1481-1489.
- Enzler MJ, Berbari E, Osmon DR. Antimicrobial prophylaxis in adults. Mayo Clin Proc. 2011;86(7):686-701.
- Thomas N, Brook I. Animal bite-associated infections: microbiology and treatment. Expert Rev Anti Infect Ther. 2011;9(2):215-226.
- Eilbert WP. 18 year old male with left hand pain. In: Weinstock MB, ed. Bouncebacks! Columbus, OH: Anadem; 2018:1-12.
The case described in this article was discussed on the HIPPO podcast: Urgent Care Reviews and Perspectives (UC RAP) by Michael Weinstock and Matthew Delaney in March 2020.
Author affiliations: Michael Weinstock, MD, Adena Health System; The Wexner Medical Center at The Ohio State University. Gabby Gostigian, MD, University of South Florida Morsani College of Medicine. Matthew Delaney, MD, University of Alabama. The authors have no relevant financial relations with any commercial interests.

Michael B. Weinstock, MD
