Published on
Zaharoula A. Viennas, MD; Julie Martin, MAEd, MMS, PA-C; Benjamin Klick, MD; Tammy Speerhas, DNP, FNP-C, RN, CEN, CME; Turaj Vazifedan, DHSc; Danielle Millspaugh, DNP, FNP-C; Jennifer Ferris, MD; Margret Bedle, MD; Lauren Paluch, DMSc, PA-C; and Theresa Guins, MD
Urgent message: Research has shown distinct differences in patterns of children presenting to emergency rooms during COVID-related lockdowns. However, data specific to urgent care have been lacking previously.
Citation: Viennas ZA, Martin J, Klick B, Speerhas T, Vazifedan T, Millspaugh D, Ferris J, Bedle M, Paluch L, Guins T. A comparison of chief complaints, specific diagnoses, and demographics of pediatric urgent care visits before and during the COVID-19 pandemic: a retrospective study. J Urgent Care Med. 2023;17(5):32-37.
Key words: COVID, pandemic, pediatric, research, urgent care
ABSTRACT
There was an increased incidence of pediatric patients who presented with injuries caused by falls not related to sports or other recreational activities, as well as for animal bites, during the early pandemic period of April 2020. Education of parents and caregivers of young children is warranted to raise awareness of the even greater potential for falls and animal bites when children are confined at home for longer than typical periods of time, as occurred with the stay-at-home government orders during the initial period of the COVID-19 pandemic.
INTRODUCTION
On March 13, 2020, the United States declared a national emergency and initiated widespread shelter-in-place orders to combat community transmission of the novel coronavirus, SARS-CoV-2. The first case of SARS-CoV-2 in the Commonwealth of Virginia was diagnosed on March 7, 2020. On March 12, a state of emergency was declared as the number of cases increased. On March 16, Governor Ralph Northam and State Health Commissioner M. Norman Oliver, MD, MA issued a public health emergency prohibiting more than 10 patrons in restaurants. Within a week, all recreation, entertainment services, fitness clubs, barbershops, and massage parlors were closed. Finally, on March 23, Governor Northam announced that all schools in Virginia would remain closed until the end of the academic year.1
Early reports from other countries noted sharp drops in the numbers of patients presenting to the emergency department.2 Likewise, early in the pandemic, the Centers for Disease Control and Prevention analyzed data from the National Syndromic Surveillance Program on the weekly number of ED visits from January 1, 2019 to May 30, 2020. The number of ED visits decreased 42% during the period of March 29 to April 25, 2020 compared with March 31 to April 27, 2019. The largest proportional declines occurred in visits by children ≤10 years of age (72% decrease) and in adolescents 11 to 14 years old (71%).3
Not only were there changes in the volumes of pediatric patients presenting to emergency departments, but also in the types of complaints proportional to the number of visits. For example, compared with the same time in 2019, in 2020 the proportion of mental health-related visits for children 5 to 11 years of age increased 24%, while those visits for teens 12 to17 years of age increased approximately 31%. During weeks 12–42, 2020 (mid-March to October), average weekly reported numbers of total ED visits by children were 43% lower compared with those during the same period in 2019.
While there are some data comparing early pandemic and prepandemic pediatric emergency room visit types, there are no data on how the COVID-19 pandemic in April 2020 impacted pediatric urgent care centers in the United States. There are also no data on the severity of illness or of the demographics of the pediatric patients presenting to urgent care centers at this time or whether children of color or ethnic minorities, typically considered vulnerable populations, were found to have more severe illness and need for a higher level of care and transfer to the pediatric ED.
Hence, in this retrospective chart analysis we examined types of chief complaints and International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes for all completed visits of all pediatric patients who presented for medical care to four pediatric urgent care centers affiliated with a children’s hospital, during both April 2019 and April 2020. Severity of illness in four subgroups that often require transfer to the ED—disorders of breathing, skin-and-soft-tissue infection (SSTI), urinary complaints, and trauma—and demographic information were further evaluated by manual chart review.
METHODS
Children’s Hospital of the King’s Daughters (CHKD) is the only freestanding children’s hospital in Virginia, and home of the region’s only Level I pediatric trauma center. CHKD serves the medical and surgical needs of children throughout coastal Virginia and northeastern North Carolina.
The urgent care centers (UCCs) are an integral part of CHKD and render services to patients from birth to <21 years of age. In April 2019, there were four UCCs open 7 days a week with a total of 7,579 completed visits. In April 2020, all four urgent care centers were operating for in-person visits from April 1 through 14. As of April 15, one of the centers converted to telehealth (TH) visits only. For the month of April 2020, compared with April 2019, there was a 70% drop in total visits, with a total of 2,291 completed visits (including the 136 completed TH encounters).
This study sought to provide understanding of what types of pediatric patient complaints and diagnoses were seen during the early pandemic period of April 2020, and whether there was a difference in type and severity of patients who presented during this time compared with the prepandemic period in April 2019. All chief complaints and ICD-10-CM discharge diagnosis codes for both time periods were reviewed and agreed upon by two investigators, with the principal investigator (PI) as the third reviewer for consensus, when necessary.
From these data, four subgroups of patients with ICD-10-CM codes, including any type of trauma-head injury, fall, motor vehicle accident, fracture, sprain, strain, laceration, bite, contusion, nonaccidental trauma, SSTI-cellulitis and abscess, urinary complaint-dysuria, hematuria, cystitis, urinary tract infection, and concern for abnormal breathing-asthma, bronchospasm, wheezing, and laryngotracheitis were further identified. Patients with these discharge diagnosis codes were further evaluated, as these patients can require a higher level of care or transport to the ED.
Additional evaluation with chart reviews for those four subgroups of patients was then undertaken. Trained investigators manually reviewed 2,635 charts that had these diagnoses from both time periods (1,816 from 2019 and 819 from 2020) for patient demographics (age, gender, race, ethnicity, insurance type) and patient outcome, with need for transfer to the ED, for hospitalization, or surgical intervention. All data were entered and stored in Research Electronic Data Capture (REDCap), the web-based application developed by Vanderbilt University.
The Institutional Review Board (IRB) of the Eastern Virginia Medical School granted IRB exemption for this study. IRB #21-03-XX-0084. Turaj Vazifedan is a statistician. He completed a statistical review and approved the methodology.
Statistical Analysis
Continuous variables are presented as mean, standard deviation (SD), median, 25th and 75th percentile. Categorical variables are presented as frequency and percentage. Mann-Whitney test was used to compare the age between 2019 and 2020. Chi-square test was used to compare differences in the rates of gender and diagnosis between 2019 and 2020. All statistical tests were performed using SPSS.26 (Chicago, IL). All statistical tests were two-sided, and p<0.05 was considered as statistically significant.
RESULTS
In April 2019, a total of 7,579 completed visits occurred. In April 2020, all four urgent care centers were operating for in-person visits from April 1-14. As of April 15, one of the centers converted to telehealth (TH) visits only. For the month of April 2020, compared with April 2019, there was a drop in total visits by 70% with a total of 2,291 completed visits, including the 136 completed TH encounters.
A total of 2,635 charts from both time periods (1,816 from 2019 and 819 from 2020) that had an ICD-10-CM diagnosis of asthma, croup, bronchospasm, wheezing, urinary complaint, SSTI such as abscess and cellulitis, and any trauma codes were then evaluated by chart review. Patient demographics (age, gender, race, ethnicity, insurance type) and patient outcome-discharge to home, transfer to any ED, transfer to the CHKD ED, hospital admission, and need for surgery were also evaluated.
Demographic variables assessed included age, gender, race, ethnicity (Hispanic, non-Hispanic Black, non-Hispanic White, non-Hispanic Asian, and non-Hispanic other) and primary payer (medical assistance, private insurance, self-pay, Tricare, other). There was a significant difference in age between 2019 and 2020, with younger patients seeking care in April 2020-median age 5.9 years vs 7.3 years in 2019.
There was no significant difference in the proportion of urgent care visits of patients who identify as a minority race or ethnicity.
In both April 2019 and 2020, patients who identified as non-Hispanic Black made up 34% and 35.3% of the visits, respectively, while patients who identified as Hispanic made up 5.3% and 4.3%, respectively. Patients who identified as non-Hispanic White made up 54.7% of the visits in both of these time periods.
Additionally, there was no significant difference in the proportion of patients based on payer type. Patients with medical assistance made up 38% of the visits in April 2019 vs 41% of the visits in April 2020. Patients with private insurance made up 42% of the visits in April 2019 vs 35% of the visits in April 2020 and patients with Tricare made up 17.8% and 21.6% of the visits in each of these time periods, respectively. Self-pay patients made up 2.0% and 1.6% of the visits, respectively.
For patients with the diagnoses noted previously, evaluated by manual chart review, there was not any significant difference in the rate of ED transfer (% difference [diff] 1.1, 95% CI (-1.0, 2.7), p=0.21), transfer to CHKD ED (% diff 6.0, 95% CI (-21.8, 10.3), p=0.65) and CHKD hospital admission (% diff 16.0, 95% CI (-6.9, 38.8), p=0.19) between April 2019 and April 2020.
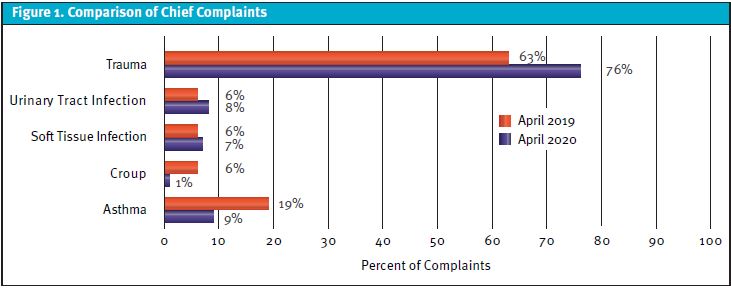
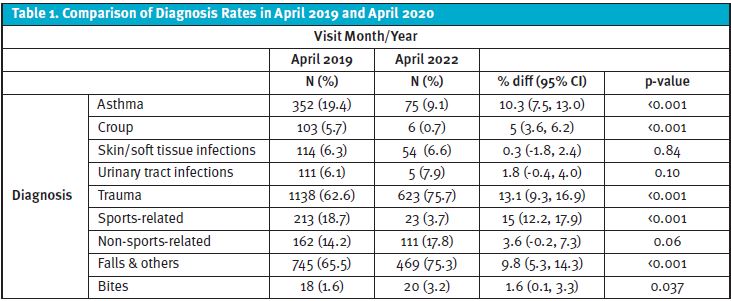
For all patients seen during April 2019, 2.17% (n=165) transferred to the CHKD ED by either EMS, the CHKD Transport Team, or via private other vehicle (POV) in April 2019, with 3.6 % transfers (n=84) in April 2020. Five patients were transported by EMS to other hospitals in April 2019 vs one patient in April 2020. Common complaints bringing patients to the urgent care in both time periods were upper respiratory symptoms, rash, abdominal complaints (vomiting, diarrhea, abdominal pain), lower respiratory complaints, soft-tissue infection, trauma, and urinary complaints. To determine if there were increases in severity of the more common complaints leading to transfer to the CHKD ED, we looked at the chief complaints as pertaining to trauma, soft-tissue infection, urinary complaint, asthma, and croup for both time periods. (See Figure 1 and Table 1.)
Trauma
Sports-related injuries included the following organized and recreational activities: basketball, baseball, softball, football, soccer, lacrosse, cheer, and dance. Non–sports-related injuries included those sustained as a result of a trampoline; any injury involving wheels, including motor vehicle-related injuries; burns; and nonaccidental trauma. Falls included those visits with a fall that did not involve either sports or non–sports-related injuries, and bite injuries were any type of human or animal bite.
There was a significantly higher number of visits for trauma-related diagnoses in 2020 compared with 2019 (% diff 13, 95% CI (9.3, 16.9) (p<0.001). However, there was a significantly lower number of sports-related injury visits in 2020 (% diff 15.0, 95% CI (12.2, 17.9), p<0.001). Visits for falls (% diff 9.8, 95% CI (5.3, 14.3), p<0.001) and bites (% diff 1.6, 95% CI (0.1, 3.3), p<0.037) were significantly higher in 2020. Falling was the top reason for injury during both time periods. (See Developing Data, page 49.)
Soft-Tissue Infection
There was no significant difference in the rate of abscesses (% diff 0.3, 95% CI (-1.8, 2.4) p=0.84), in gender (% diff 5.2, 95% CI (-23.1, 32.0), p=0.90) or race (% diff 4.1, 95% CI (-34.6, 26.3), p=0.98) for those patients that needed an abscess drained in April 2020 vs April 2019.
Urinary Complaint
There was no significant difference in the rate of those patients diagnosed with a UTI in April 2019 compared with April 2020 (% diff 1.8, 95% CI (0.4, 4.0), p=0.10). Diagnosis of a UTI was based on urine culture results with ≥50,000 CFU/mL of a solitary organism on a clean-catch urine and ≥10,000 CFU/mL of a solitary uropathogen on a catheterized specimen considered as positive, respectively. In addition, there was not any significant difference in the rate of males diagnosed with UTI in 2019 vs 2020 (% diff 2.9, 95% CI (-9.4, 15.0) p=0.78). There was not any significant difference in the rate of White patients diagnosed with a UTI in 2019 vs 2020 (% diff 14.0 95% CI (-1.2, 29.0), p=0.09). There was not any significant difference in the age of those diagnosed with UTI in 2019 vs 2020 (mean diff 0.16 95% CI (-1.8, 1.4), p=0.84).
Asthma and Croup
There were significantly lower numbers of visits resulting in a diagnosis of asthma (including wheezing and bronchospasm) (p <0.001) and croup (p<0.001) in 2020 compared with 2019.
Asthma, bronchospasm, and croup were differentiated from viral upper respiratory infections because patients with these diagnoses are at risk for respiratory distress and have potential for needing a higher level of care.
DISCUSSION
Early in the pandemic, in March and April 2020, stay-at-home orders were in place for Virginia. Several pediatric offices in southeastern and coastal Virginia were not seeing febrile children or those with respiratory illnesses, referring those children to the urgent care centers affiliated with the only pediatric hospital in the area. In this retrospective chart analysis, we examined the types of patients who presented for care to four pediatric urgent care centers based on chief complaint and ICD-10-CM during April 2020 and compared them with those who presented in the prepandemic period in April 2019.
There was a younger patient cohort who presented for care in April 2020. The percentage of the total visits was higher for fall injuries not related to sports and non-sports recreational activities and bite injuries during this early pandemic period, as well. Visits for respiratory illnesses such as asthma and croup were noted at lower rates compared with April 2019, similar to what has been shown in other studies.4-7
LIMITATIONS
Limitations of this analysis were that classification into the subcategories (asthma, croup, SSTI, urinary complaints, and trauma) relied on the ICD-10-CM codes with the potential for misclassification. However, each chart was reviewed by two separate reviewers who looked at the ICD-10-CM codes as well as the chief complaint, with the third reviewer as the tie breaker if there was discordance. In addition, these data reflect those pediatric patients who sought treatment in the urgent care and do not reflect those who sought treatment in the emergency department, or who did not seek treatment at all. Hence, there may be an underestimation of specific diagnoses or their incidence during this time. However, other studies have shown a decrease in the pediatric ED visits during April 2020 and, as noted previously, many primary care offices were not offering in-person care for ill patients during this time.8
The study period compared patient visits from April 2019 and April 2020. April was chosen because it was the first full month of the COVID-19 pandemic lockdown. However, it should be noted that these data may not represent the variety of chief complaints that bring patients into urgent care throughout all months of the year.
In the early months of SARS-CoV-2, the greatest decline in ED visits nationwide was in the pediatric population.3 There is little data available from urgent care centers that see both adult and pediatric patients. Our data may not apply to all urgent care centers, especially those that also treat adults.
Finally, this retrospective analysis reflects pediatric urgent care data from one pediatric hospital’s catchment area in southeastern Virginia and may not be generalizable to what occurred elsewhere in the U.S. during this time. However, this catchment area serves children in rural, suburban, and urban communities. In addition, this retrospective analysis was powered by the large sample size and with complete assessment of age, gender, race, ethnicity, and primary payer information. This assessment did not show a difference in the gender, race, ethnicity, or types of payers of the patients seeking care during these two time periods.
CONCLUSIONS
Our analysis of visits to four pediatric urgent care centers affiliated with a children’s hospital in Virginia showed that there was an increased incidence of pediatric patients who presented with injuries caused by falls not related to sports or other recreational activities and for care of primarily animal bites during the early pandemic period of April 2020 compared with April 2019 (prepandemic period). Many of these falls and bite injuries occurred while at home, in younger children and with family pets, respectively. Unintentional falls were the leading cause of nonfatal ED visits in the U.S. in 2019, for infants and children ≤14 years of age (most recent year).9
Education of parents and caregivers of young children is warranted to raise awareness of the even greater potential for falls and animal bites when children are confined at home for longer than typical periods of time, as occurred during April 2020 with stay-at-home government orders during the initial period of the COVID-19 pandemic. More children accessed care for injuries at our urgent care facilities during the first month of the pandemic compared with the same month prepandemic. If future stay-at-home orders are instituted, resources including access to timely radiology imaging and interpretation, splinting materials, sutures, and other medical supplies related to wound cleaning and care need to be prioritized.
REFERENCES
- Virginia Timeline for Response to COVID-19. Virginia’s First Congressional District Website. Available at: https://wittman.house.gov/coronavirus/virginia-timeline.htm. Accessed September 1, 2021.
- Wong LE, Hawkins JE, Langness S, et al. Where are all the patients? Addressing COVID-19 fear to encourage sick patients to seek emergency care. NEJM Catal Innov Care Deliv. May 14, 2020.
- Hartnett KP, Kite-Powell A, Devies J, et al. Impact of the COVID-19 pandemic on emergency department visits- United States, January 1, 2019- May 30, 2020. MMWR Morb Mortal Wkly Rep. 2020; 69(23):699-704.
- Simoneau T, Grego KF, Hammond A, et al. Impact of the COVID-19 pandemic on pediatric emergency department utilization for asthma. Ann Am Thorac Soc. 2021; 18(4):717-719.
- Arsenault S, Hoofman J, Poowuttikul P, Secord E. Sustained decrease in pediatric asthma emergency visits during the first year of the COVID-19 pandemic. Allergy Asthma Proc. 2021;42(5):400-402.
- Davies G, Alsallakh MA, Sivakumaran S, et al. Impact of COVID-19 lockdown on emergency asthma admissions and deaths: national interrupted time series analyses for Scotland and Wales. Thorax. 2021;76(9):867-873.
- Huh K, Kim YE, Ji W, et al. Decrease in hospital admissions for respiratory diseases during the COVID-19 pandemic: a nationwide claims study. Thorax.2021;76(9):939-941.
- Kostopoulou E, Gkentzi D, Papasotiriou M, et al. The impact of COVID-19 on paediatric emergency department visits. A one-year retrospective study. Pediatr Res. 2021;1-6.
- Centers for Disease Control and Prevention. CDC Web-based Injury Statistics Query and Reporting System. Ten leading causes of nonfatal emergency department visits, United States. Available at: https://wisqars.cdc.gov/cgi-bin/broker.exe. Accessed January 17, 2022.
Manuscript submitted April 6, 2022; accepted October 18, 2022.
Acknowledgement: The authors acknowledge the support ofAngela Robertson, BS, CPC, Director of Urgent Care Services, Children’s Hospital of the King’s Daughters in the creation of this article.[HF1]
Author affiliations: Zaharoula A. Viennas, MD, Department of Pediatrics, Eastern Virginia Medical School; Children’s Hospital of the King’s Daughters Urgent Care Services. Julie Martin, MAEd, MMS, PA-C, Children’s Hospital of the King’s Daughters Urgent Care Services. Benjamin Klick, MD, Department of Pediatrics, Eastern Virginia Medical School; Children’s Hospital of the King’s Daughters Urgent Care Division; CHKD Urgent Care Quality and Guidelines Committee. Tammy Speerhas, DNP, FNP-C, RN, CEN, CME, Department of Pediatrics, Eastern Virginia Medical School; School of Nursing, Old Dominion University; Children’s Hospital of the King’s Daughters Urgent Care Services. Turaj Vazifedan, DHSc, Department of Pediatrics, Eastern Virginia Medical School, Children’s Hospital of the King’s Daughters. Danielle Millspaugh, DNP, FNP-C, Children’s Hospital of the King’s Daughters Urgent Care Services. Jennifer Ferris, MD, Children’s Hospital of the King’s Daughters Urgent Care Services. Margret Bedle, MD, Children’s Hospital of the King’s Daughters Urgent Care Services. Lauren Paluch, DMSc, PA-C, Eastern Virginia Medical School Physician Assistant Program. Theresa Guins, MD, Children’s Specialty Group Division of Urgent Care; Children’s Hospital of the King’s Daughters Urgent Care Services; Eastern Virginia Medical School.