Published on
Differential Diagnosis
- Benign early repolarization
- Hypothermia
- Acute pericarditis
- ST-elevation Myocardial Infarction (STEMI)
- Brugada syndrome
Diagnosis
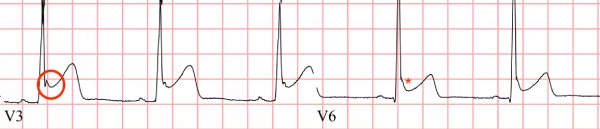
The ECG reveals a normal sinus rhythm with a rate of 60 beats per minute. There is diffuse, concave-up ST-segment elevation particularly in precordial (V2-6) and limb leads (II, III, aVF), without reciprocal changes. There is J-point notching and slurring of the ST segment, particularly in the precordial leads. This patient was diagnosed with benign early repolarization.
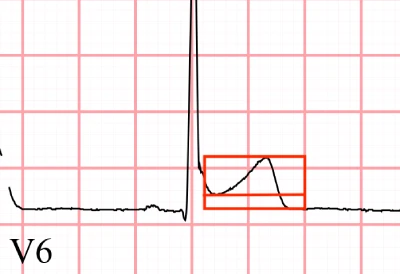
Commonly referred to as “benign” early repolarization, or the “J wave pattern,” this diagnosis features diffuse ST elevations that are most pronounced in V2-V5, with notching or slurring at the J-point (Figure 2), and an ST elevation-to-T wave height ratio <0.25 in V6 (Figure 3). This ECG diagnosis also characteristically has concordant T waves (going in the same direction as the QRS) and lacks reciprocal ST depressions.1
Differentiating early repolarization from other conditions requires a clinician to look at the big picture—the clinical presentation, additional findings on the ECG, and previous ECGs, if available. Concerning diagnoses to differentiate from benign early repolarization include:
- STEMI: Reciprocal changes are more pronounced and convex (“tombstone” morphology”) ST-elevations are expected.
- Pericarditis: Also has generalized ST-elevations, but with PR depressions and an ST-elevation to T wave ratio >0.25.2
- Hypothermia: J-point notching is seen in hypothermia, but typically without ST elevation
- Brugada syndrome: ST-elevation specifically in V1 and V2 (with an R R’ pattern)
There is currently no consensus on the etiology of the early repolarization pattern. Recent studies have found subgroups of patients with a J wave that also have increased risk of ventricular dysrhythmias and sudden cardiac death. However, these cases are rare and most cases of J point elevation are considered benign, particularly in the absence of personal or family history of malignant arrhythmia.3
Learnings/What to Look for
- The differential for ST elevation is broad and includes not only STEMI, but early repolarization, pericarditis, Brugada syndrome, and hypothermia. When presented with an ECG with ST-elevation, consider the whole clinical picture
- Early repolarization is common in patients under the age of 50. Over 50, consider that ischemia may be a more likely cause of ST elevation. If there is a question, default for the more serious diagnosis
- When diagnosing early repolarization, look for diffuse ST elevations that are most pronounced in V2-V5, notching or slurring at the J-point, an ST elevation-to-T wave ratio <0.25, concordant T waves, and a lack of reciprocal ST depressions.
Pearls for Urgent Care Management
- Typically, early repolarization is benign and requires no treatment or follow-up. However, don’t forget to consider the patient’s symptoms and ask about risk of ventricular dysrhythmias and sudden cardiac death
- If the diagnosis is unclear, the symptoms are concerning, or the patient is more than 50 years old, transfer to an emergency department is appropriate
References
- Mehta MC, Jain AC, Mehta A. Early repolarization. Clin Cardiol. 1999;22(2):59-65.
- Ginzton LE, Laks MM. The differential diagnosis of acute pericarditis from the normal variant: New electrocardiographic criteria. Circulation. 1982;65(5):1004-1009.
- de Bliek EC. ST elevation: differential diagnosis and caveats. A comprehensive review to help distinguish ST elevation myocardial infarction from nonischemic etiologies of ST elevation. Turk J Emerg Med. 2018;18(1):1-10.