Published on
Urgent message: While healthcare disparities have been studied in several healthcare settings, it is unclear whether they persist in urgent care. This study may serve as a quality improvement tool to assess whether these disparities persist in an urgent care clinic.
Derrick Murcia and Lindsey Fish, MD
Citation: Murcia D, Fish L. Evaluation of healthcare disparities in urgent care: a case example for bacterial pneumonia. J Urgent Care Med. 2022;16(4):23-27. Epub ahead of print September 14, 2021.
ABSTRACT
Background
Bacterial pneumonia is an illness commonly seen across urgent care clinics. Despite several studies that have identified healthcare disparities in treating bacterial pneumonia in general, research is needed to verify if these disparities exist in the urgent care setting. This study describes a quality improvement tool that uses bacterial pneumonia as an example to check for disparities within a single urgent care center.
Methods
Medical records from a single urgent care clinic were screened to a set of inclusion and exclusion criteria from January 1, 2017 to December 31, 2019 using the following ICD-10 codes: J12.X, J13.X, J14.X, J15.X, J16.X, J17.X, and J18.X. Data were also pulled for 14-day return rates following discharge from the urgent care clinic. Patient visits were classified into two groups: treatment-concordant and treatment-discordant, based on whether they received first-line antibiotic treatment. Fisher’s exact test was then used to make comparisons across several categorical variables.
Results
A total of 245 visits with bacterial pneumonia as the primary diagnosis were identified, with 233 of these visits being unique patients. No significant differences were observed between the treatment-concordant and treatment-discordant cohorts with respect to gender (p=>0.9999), age (p=0.2346), race (p=0.4464), ethnicity (p=>0.9999), insurance status (p=0.8765), and return visit to any healthcare center (p=0.3538). No significant differences were also observed when distinguishing between healthcare facility type—primary care (p=0.2617), specialist (p=0.4637), urgent care (p=0.1016), emergency department (p=0.3940), and inpatient setting (p=0.2277).
Conclusion
This study provides a rapid method to identify healthcare disparities for many illnesses commonly seen in urgent care clinics. While there were no statistically significant findings for the treatment of bacterial pneumonia at this urgent care clinic, evidence suggests that excellent antibiotic stewardship may play a role in mitigating these types of healthcare disparities.
INTRODUCTION
Bacterial pneumonia is defined as a lung infection that is commonly caused by S pneumoniae. Annual incidence is approximately 5 million people, with 75% of cases being treated at an outpatient site.1 Management and treatment may vary depending on clinical setting and location.
Empiric antibiotic treatment is a key hallmark for management of bacterial pneumonia.2 Previous studies suggest racial and ethnic disparities are evident in the incidence and management of this illness.3,4 However, there are limited studies which have investigated the incidence, management, or outcomes of bacterial pneumonia based on socioeconomic factors specifically.3–12
Together, these studies suggest four major findings:
- Bacterial pneumonia occurs at a higher rate in racial/ethnic minority patients when compared to Caucasians.3,4 However, these studies are limited in generalizability to the Hispanic population because some medical records did not specify ethnicity.
- It is unclear if hospitals with lower quality of care indicators exacerbate these racial/ethnic disparities.4,6,9,11,12
- Vaccination administration rates with the 23-valent pneumococcal polysaccharide vaccine are lower among nonwhite adults compared to Caucasians.3,4,7
- Racial/ethnic minority patients experience delays in antibiotic administration and are less likely to receive some guideline-concordant treatments for pneumonia.4 There is concern that this may cause higher complication and mortality rates among racial/ethnic minority patients.
The Federico F. Peña Southwest Urgent Care Clinic (PUCC) opened in April of 2016 and is uniquely located within the Federico F. Peña Southwest Family Health Center, a Federally Qualified Health Center (FQHC). It is affiliated with Denver Health and Hospital, a safety net urban hospital with associated FQHC community health clinics located throughout metro Denver. This urgent care clinic resides at the intersection of four Denver neighborhoods. All of these neighborhoods have a high concentration of medically underserved populations: 20% of the population is comprised of non-English speaking adults, 70% identify as Latinx, 51% of households are low income, and 20% of the population is in poverty.13 The clinic additionally draws patients from all across the Denver metro area, therefore serving a racially and economically diverse population. Integration within the Federico F. Peña Southwest Family Health Center allows the urgent care clinic to provide care to patients regardless of age, language, insurance status, or ability to pay. The urgent care clinic is financially supported by Denver Health, which includes federal grant funding through the Health Resources and Services Administration (HRSA) Health Center Program. On average, the PUCC sees approximately 25,000 visits annually.
Antibiotic stewardship programs are an effective strategy to minimize unnecessary cost and establish a universal guideline for treating illnesses secondary to bacteria.14 In general, these programs require two things: agreement on best clinical practices and accessibility to providers. At Denver Health, a smartphone application that provides an electronic antibiogram along with recommendations was developed and implemented in 2014. It has demonstrated increase use over the years, suggesting adherence to guideline-concordant treatments.15
No studies, to the best of our knowledge, have investigated whether these healthcare disparities regarding the evaluation and treatment of bacterial pneumonia persist in urgent care centers (UCCs). We performed a retrospective cohort study that investigated whether Hispanic and non-Hispanic patients seen at the Peña Southwest Urgent Care Clinic received treatment according to Denver Health’s antibiotic guidelines. Furthermore, we determined if patients who received guideline-discordant therapy had a higher 14-day return rate with respect to patients who received guideline-adherent therapy. We believe that this evaluation model can be applied to UCCs across the United States and utilized as a tool for quality improvement.
METHODS
All methods were approved by the Denver Health Quality Improvement Review Committee, a Colorado Multiple Institutional Review Board quality committee.
Study Characteristics
This is a retrospective cohort study that examined provider adherence to antibiotic guidelines for patients diagnosed with bacterial pneumonia at PUCC. Medical records were screened to a set of inclusion and exclusion criteria from January 1, 2017 to December 31, 2019 using the following ICD-10 codes: J12.X, J13.X, J14.X, J15.X, J16.X, J17.X, and J18.X. Inclusion criteria consists of the following: adults 18 years or older and with the above diagnoses. Exclusion criteria consist of the following: patients less than 18 years old, pregnant patients, patients with an allergy to doxycycline, patients who were admitted to the hospital, and medical records not indicating race/ethnicity. Medical records were stratified into two cohorts and compared against different categorical variables (Table 1). These groups are defined as guideline-adherent (prescribed 100 mg doxycycline twice daily by mouth for 5 days) and guideline-discordant (any other prescription). Absolute counts of return visits (<14 days) were also determined based on location of return visit.
Statistical Analysis
All statistical analysis was performed in GraphPad Prism (version 8.4.3). Fisher’s exact test was employed across different categorical variables (demographics and return visits) to identify if there was any significant deviation from the institution’s treatment guidelines for bacterial pneumonia. Two-sided p-values are reported. If needed, sub variables were grouped in order to increase power when making comparisons. Bar graphs were created to illustrate these comparisons.
RESULTS
Population Characteristics
A total of 245 urgent care visits that led to a primary diagnosis of bacterial pneumonia were included in this study. Of the 245 visits, 233 were identified to be unique patients. Demographic information and return visit (<14 days) data for guideline-adherent and guideline-discordant information can be viewed in Table 1.
Table 1. Patient Demographics
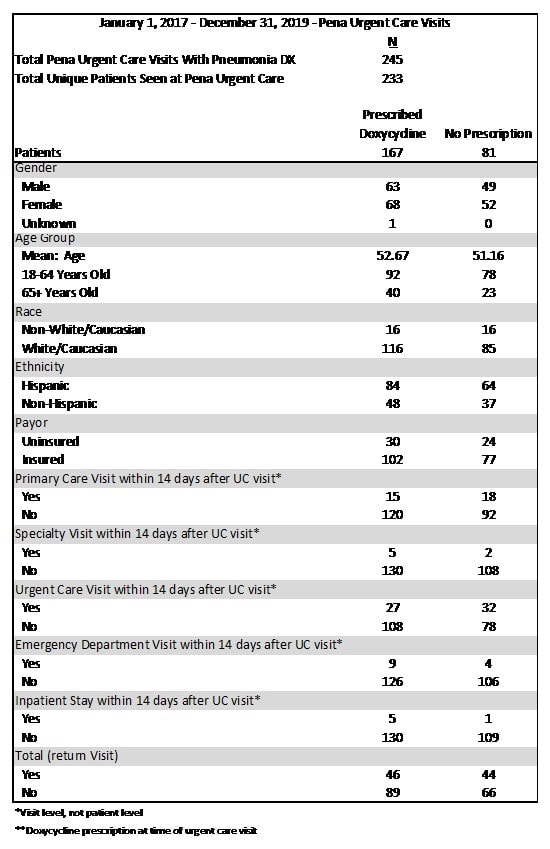
Cohort Comparisons with Demographic Information and Return Visit Data
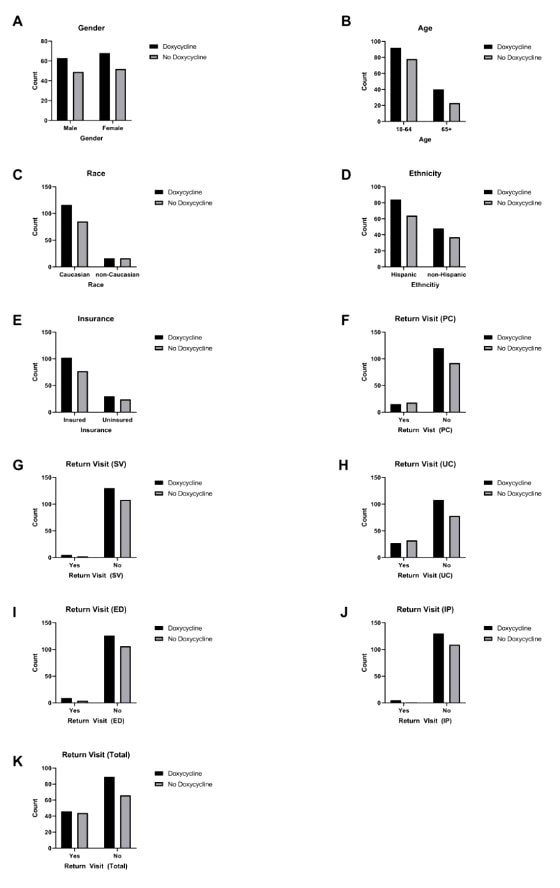
Healthcare disparities among both cohorts were evaluated using Fisher’s exact test to determine if demographic data corresponded to a significant difference between both groups (Figure 1). No significant differences were observed among cohorts with respect to gender (p=>0.9999), age (p=0.2346), race (p=0.4464), ethnicity (p=>0.9999), insurance status (p=0.8765), and return visit to any healthcare center (p=0.3538). No significant differences were observed when differentiating between healthcare facility type—primary care (p=0.2617), specialist (p=0.4637), urgent care (p=0.1016), emergency department (p=0.3940), and inpatient setting (p=0.2277).
Figure 1. Fisher’s Exact Test Comparisons
DISCUSSION
UCCs within the United States have experienced unprecedented growth in recent years (irrespective of the COVID-19 pandemic), resulting in centers operating in areas with a high population density of minority residents.16 However, few studies have used data acquired from UCCs to investigate whether healthcare disparities exist in this clinical setting. Here, we used information from medical records to demonstrate a rapid, systematic method to check for disparities in treating bacterial pneumonia. Pneumonia was selected because of previous studies indicating a health disparity, high mortality rate, and complication rate as it is the ninth leading cause of death and third leading cause for hospitalization in the United States.17
As shown in the results, we found no differences between the guidelines-adherent and guideline-discordant groups in the treatment of bacterial pneumonia. No statistically significant difference was found based on gender, age, race, ethnicity, insurance status, or return visit. We suspect that the use of an electronic antibiogram, along with clear guidelines, helped reduce providers’ implicit bias when prescribing medications. Previous studies have demonstrated that the use of an antimicrobial stewardship program is useful for providing systematically sound care while minimizing incorrect medication administration and unnecessary expenses.14,15,18
This study presents a model for quality improvement measures in the urgent care setting. There are several advantages of this quality improvement model.
The first advantage is that this model can be used as a tool to identify if the UCC is following guideline-adherent therapies. This method can be integrated into other quality improvement measures to acquire an accurate representation of UCC performance.
The second advantage of this model is that it can be applied universally to any UCC and disease state. Although bacterial pneumonia was used in this study, this model can use data from other diseases to identify if there is a deviation from guideline recommended therapy.
Third, the method can be performed quickly as it only requires absolute counts for data and basic software for statistical analysis.
LIMITATIONS
With these advantages in mind, there are some limitations. The UCC must have sufficient medical records in the category of interest to power the analysis. This limits the analysis to relatively older UCCs, as newer UCCs may not have enough data for this model to detect a significant difference. Another limitation is that it requires a clear definition for the first-line treatment of the disease. In this example, 100 mg doxycycline twice daily by mouth for 5 days was established as the gold standard. However, there are some diseases that do not have established guidelines as first-line for treatment, which therefore can limit the use of this model.
CONCLUSIONS
UCCs have recently experienced a massive growth within the United States, but few studies have analyzed data from these healthcare sites, specifically data looking at healthcare disparities. Here, we used a simple retrospective cohort study focused on bacterial pneumonia to demonstrate a rapid method to check for disparities. This model could be easily applied to other urgent care clinic settings and to other disease states as a quality improvement method. In this study, no disparities were found in the treatment for bacterial pneumonia, which we suspect is a result from mitigated implicit bias in the treatment of bacterial pneumonia due to clear guidelines and excellent antibiotic stewardship.
REFERENCES
- Harnett G, Sellers J. Urgent care evaluation of pneumonia. J Urgent Care Med. 2017;11(5):11-18.
- Prina E, Ranzani OT, Torres A. Community-acquired pneumonia. Lancet. 2015;386:1097-1108.
- Burton DC, Flannery B, Bennett NM, et al. Socioeconomic and racial/ethnic disparities in the incidence of bacteremic pneumonia among US adults. Am J Public Health. 2010;100(10):1904-1911.
- Hausmann LRM, Ibrahim SA, Mehrotra A, et al. Racial and ethnic disparities in pneumonia treatment and mortality. Med Care. 2009;47(9):1009-1017.
- Downing NS, Wang C, Gupta A, et al. Association of racial and socioeconomic disparities with outcomes among patients hospitalized with acute myocardial infarction, heart failure, and pneumonia: an analysis of within- and between-hospital variation. JAMA Netw Open. 2018;1(5):e182044.
- Gaskin DJ, Spencer CS, Richard P, Anderson GF, Powe NR, LaVeist TA. Do hospitals provide lower-quality care to minorities than to whites? Health Aff. 2008;27(2):518-527.
- Mayr F, Yende S, D’Angelo G, et al. Do hospitals provide lower quality of care to black patients for pneumonia? Crical Care Med. 2010;38(3):759-765.
- Mortensen EM, Cornell J, Whittle J. Racial variations in processes of care for patients with community-acquired pneumonia. BMC Health Serv Res. 2004;4:1-7.
- Fine JM, Fine MJ, Galusha D, et al. Patient and hospital characteristics associated with recommended processes of care for elderly patients hospitalized with pneumonia results from the medicare quality indicator system pneumonia module. JAMA Intern Med. 2002;162(7):827-833.
- Jha AK, Orav EJ, Zheng J, Epstein AM. The characteristics and performance of hospitals that care for elderly hispanic Americans. Health Aff. 2008;27(2):528-537.
- Jha AK, Orav EJ, Li Z, Epstein AM. Concentration and quality of hospitals that care for elderly black patients. JAMA Intern Med. 2007;167(11):1177-1182.
- Hasnain-Wynia R, Baker DW, Nerenz D, et al. Disparities in health care are driven by where minority patients seek care examination of the hospital quality alliance measures. JAMA Intern Med. 2007;167(12):1233-1239.
- Denver Metro Data: Neighborhood Summaries. Published 2017. Available at: https://denvermetrodata.org/neighborhoods. Accessed May 25, 2020.
- Feiring E, Walter AB. Antimicrobial stewardship: a qualitative study of the development of national guidelines for antibiotic use in hospitals. BMC Health Serv Res. 2017;17(1):1-11.
- Young HL, Shihadeh KC, Skinner AA, et al. Implementation of an institution-specific antimicrobial stewardship smartphone application. Proc Int Astron Union. 2018;39(8):986-988.
- Le ST, Hsia RY. BMJ open community characteristics associated with where urgent care centers are located: A cross-sectional analysis. BMJ Open. 2016;6(4):1-6.
- Rider AC, Frazee BW. Community-Acquired Pneumonia. Emerg Med Clin North Am. 2018;36(4):665-683.
- Jenkins TC, Haukoos JS, Young HL, et al. Patterns of use and perceptions of an institution-specific antibiotic stewardship application among emergency department and urgent care clinicians. Infect Control Hosp Epidemiol. 2019;41(2):212-215.
Author affiliations: Derrick Murcia, University of Colorado School of Medicine. Lindsey Fish, MD, Denver Health/University of Colorado. The authors have no relevant financial relationships with any commercial interests.

Lindsey E. Fish, MD
