Published on
Urgent message: Response to a needlestick with potential for HIV exposure requires understanding of both state laws on HIV testing and the latest USPSTF guidelines for post-exposure management.
MAYA HECK, MS-2 and JOHN SHUFELDT, MD, JD, MBA, FACEP
Two police officers arrive at your urgent care site with a handcuffed, bloodied prisoner. One officer tells you that the person in custody “spit on me” during the altercation. The officer goes on to tell you that the suspect is an intravenous drug abuser and believed to be infected with HIV. The officer is requesting a “blood test” and wants the suspect tested as well because, according to the officer, if the suspect is “positive” the officer will file different charges and wants to receive prophylaxis to prevent sero-conversion. The suspect refuses to be tested and although a bit “stunned” from being tazed, seems to be competent to refuse. What do you do? After the safety of the source patient is ensured, the health care worker potentially exposed to HIV should immediately flush out his or her wound or skin site.1
Initial management of exposure
- Exposed mucous membranes should be flushed with tap
- Exposed eyes should be flushed with sterile water or eye irrigant when
- Although antiseptics are not known to reduce inci- dence of infection, they can be used to flush the wound.
- The exposed health care worker should notify his or her supervisor so the exposure can be reported and properly evaluated according to Centers for Disease Control and Prevention (CDC) guidelines (see below).
The management of occupational exposures should be given high priority and treated as urgent or emergent, depending on the circumstance.
A note about counseling
Because occupational exposures to blood-borne pathogens can elicit a strong stress reaction, the importance of counseling for health care workers who have occupational exposures should not be underestimated. Counselors should be ready to openly discuss the health care worker’s recollection of the event and any relevant past traumatic experiences, provide information on stress reactions, provide information to his or her support system, and help reintegrate the health care worker back into the occupational environment. In addition, a thorough examination of the health care worker’s practices for sharp instrument—including handling and disposing is important to prevent future accidents.2
Not only does counseling help to ease anxiety for the exposed health care worker and his or her family, but it may also increase adherence to chemoprophylaxis regimes.3 If knowledgeable counselors are able to maintain close personal contact and discuss chemoprophylaxis and potential adverse side effects, a patient’s adherence to the regime is likely to be enhanced.
HIV
The average risk of HIV transmission is approximately 0.3% among health care workers following accidental needlestick involving an HIV-infected source patient with- out post-exposure chemoprophylaxis. The risk with a mucous-membrane exposure is approximately 0.09%.3 These risks are significantly lower than the risk of acquiring HCV or HBC from a similar injury.3 According to the CDC, there were 57 documented cases of occupational HIV transmission to health care workers in the Unit- ed States through December 2001, and no confirmed cases have been reported since 1999. Occupational transmission of HIV is reported in the Centers for Disease Control and Prevention (CDC) HIV Surveillance Report.3
Pre-exposure Prophylaxis. Currently pre-exposure prophylaxis for HIV is not available.
Post-exposure Prophylaxis. Within hours of exposure, the health care worker and source should be evaluated and tested for HIV at baseline to establish infection status. While the risk of transmission from an occupational exposure to a source patient with an undetectable serum viral load is thought to be very low, post exposure prophylaxis (PEP) should still be considered.4 In 1997, the CDC Needlestick Surveillance Group published findings from a study looking at the risk of HIV transmission among health care workers who sustain a needlestick injury.3 It was reported that zidovudine (ZDV) as PEP reduced the risk of HIV transmission by 81%.3 Now, antiretroviral (ARV) agents from six classes of drugs are available for treatment of HIV infection. These agents include the nucleoside reverse transcriptase inhibitors (NRTIs), nonnucleoside reverse transcriptase inhibitors (NNRTIs), protease inhibitors (PIs), an integrase strand transfer inhibitor (INSTI), and a chemokine (C-C motif) receptor 5 (CCR5) antagonist.
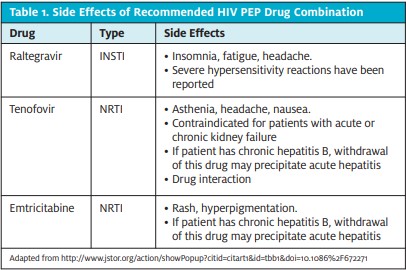
The US Public Health Service (USPHS) no longer rec- ommends that the severity of exposure (i.e. percutaneous versus large bore) be used to determine the number of drugs to be offered in an HIV PEP regimen, and a regi- men containing 3 (or more) ARV drugs is now recom- mended routinely for all occupational exposures to HIV.4 The recommended PEP regimens include those consisting of a dual NRTI backbone plus an INSTI, a PI (boosted with ritonavir), or a NNRTI. The preferred regimen includes raltegravir (Isentress; RAL) 400 mg PO twice daily plus Truvada, 1 PO once daily and tenofovir DF [Viread; TDF] 300 mg + emtricitabine [Emtriva; FTC] 200 mg.4
According to the National Surveillance System for Health care workers (NaSH) and the HIV Post-exposure Registry, about half of health care workers on PEP experience adverse symptoms such as nausea, malaise, headache, anorexia, and headache. In addition, approximately one-third discontinue PEP because of these symptoms.3 To encourage a health care worker to com- plete the regimen, medications should be selected to optimize side effect and toxicity profiles and ensure a convenient dosing schedule.
Management of PEP Toxicity
If PEP was administered, the health care worker should be monitored for drug toxicity at baseline and at 2 weeks after initiation of treatment.4 Throughout the course of PEP, an evaluation of acute symptoms and laboratory tests, including a complete blood count and renal and hepatic function tests, should be obtained. Considerations of medical conditions and drug interactions are also important; for example, monitoring a diabetic patient for hyperglycemia who is taking a protease inhibitor.4 The health care worker should be advised that reporting symptoms such as rash, fever, abdominal pain, pain on urination, or change in urine color, yellowing of the skin or whites of the eyes, or symptoms of hyperglycemia should not delayed because these may be a sign of toxicity.4 Obtaining a complete history along with all alternative and traditional medications will help minimize adverse side effects and drug toxicity with PEP treatment.
Table 1 illustrates the potential side effects of the newest 3-drug PEP regimen recommended by the USPHS.
Special Considerations for Pregnant/ Breastfeeding Health Care Workers
The risk of HIV transmission is a threat to both the mother and the fetus or infant because the risk of mother-to-child trans- mission is increased during the acute phase of infection.4 Therefore, considerations in offering PEP to a pregnant or breastfeeding health care worker should involve counsel- ing and discussion with her health care provider regarding the potential risks of PEP. These risks depend on the duration of drug exposure, as well as the type and dosage. Stavudine and didanosine treatment should be avoided throughout gestation because they have been reported to cause fatal and nonfatal lactic acidosis. Similarly, in uteroefavirenz treatment in primates has been shown to result in CNS defects and it is recommended to avoid that drug in the first trimester.4 In addition, ARV drug levels in breast milk can vary among drugs. Lamivudine is found at high levels in milk, whereas PIs and tenofovir have limited penetration. Prolonged maternal ARV drug use during breastfeeding may be associated with infant hematologic toxicity.4 To completely reduce the risk of transmission, the health care worker may want to consider stopping breastfeeding. Because of the complexity of the risks and benefits of receiving HIV PEP while pregnant or breastfeeding, expert consultation is recommended.
Post-exposure prophylaxis (PEP) for HIV should be started immediately and continued for 28 days. An updated recommendation from the USPHS is that if a newer fourth-generation combination HIV p24 antigen-HIV antibody test is utilized for follow-up HIV test- ing of an exposed health care worker, HIV testing can be concluded 4 months after exposure.4
Expert consultation from an infectious disease special- ist is advised under the following circumstances: delayed (later than 72 hours) exposure report, unknown source, known/suspected pregnancy in exposed person, known/suspected resistance of the source virus to antiretroviral agents, or serious medical illness in exposed person.4
Disease-specific follow up
For HIV exposure, disease-specific follow up consists of repeat HIV testing at 6 weeks, 3 months, and 6 months following exposure. Testing also should be done at 12 months for individuals who are HIV/HCV coinfected. If PEP is administered, monitoring of live function tests should be done. Individuals who have been exposed to HIV should refrain from donating blood or plasma and they should be offered counseling.
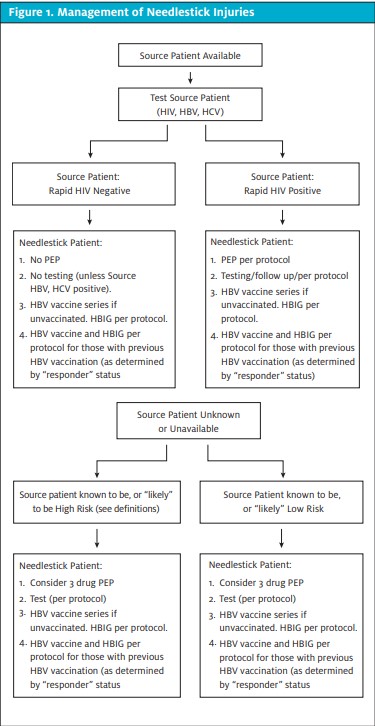
The algorithm in Figure 1, which also appears in Part 1 of this article in the November issue, provides an overview of management of needlestick injuries. The National Clinicians’ Post-Exposure Prophylaxis Hotline is a 24/7 resource that offers advice on treatment and follow-up options. Call 1-888-448-4911 or visit http://www.ucsf.edu/ hivcntr/PEPline.
Conclusion
To return to the scenario we presented at the beginning of this article, are blood tests necessary and/or permissible for the exposed officer and suspect? Alone, saliva is not considered a fluid through which HIV is transmitted. However, if infected blood is also present in the saliva, then this mixture may be infectious. In addition, the saliva-blood mixture must have been “spit” directly into the officer’s eyes, mouth or open wound for an infectious exposure. Obtaining a thorough history will help guide your clinical judgment as to whether the officer was exposed to HIV and/or other blood-borne pathogens.
The next step in medical management depends on the state in which you practice, because states have different laws regulating the permission of involuntary HIV testing. For example, in Connecticut, there are four circumstances in which HIV testing without informed consent is allowed; one is occupational exposure. Connecticut law permits a nonconsensual “HIV-related test” of the source of a “significant exposure” to HIV which occurs during a person’s occupational duties.5 As the law reads, a “significant exposure” is “a parenteral exposure such as a needlestick or cut, or mucous membrane exposure such as a splash to the eye or mouth, to blood or a cutaneous exposure involving large amounts of blood or prolonged contact with blood, especially when the exposed skin is chapped, abraded, or afflicted with dermatitis.” In order to obtain this test, the health care worker must:
- Document the occurrence of a significant occupational expo- sure and complete an incident report within 48
- Have a negative baseline HIV test within 72
- With the help of a physician, have attempted to obtain and have been refused voluntary consent from the
- Be able to take meaningful immediate action that otherwise could not be taken without the source test results (i.e. start pro- phylactic regimen).
- Be evaluated by an “exposure evaluation group,” which is defined as three impartial health care providers, one of whom must be a physician, to determine that the above criteria are 5
If the source is in a health or correctional facility, a blood sample can be obtained in that location; if the source is not in such a facility, then the health care worker can seek a court order for testing. Under Con- necticut law, the employer must pay the cost of the HIV test.
If there is legal uncertainty, and through a comprehensive history it is determined that the officer was indeed at risk of acquiring HIV from the suspect, it is recommended to initiate the 3-drug regimen of ARV agents. Given the suspect’s competent refusal to be tested, you must base your decision on your high level of suspicion that the suspect was infected with HIV.
This scenario would be treated similarly to a situation in which the infection status of the source was unknown. At this time, it is also recommended to obtain the baseline tests for HCV as outlined above. In addition, obtaining a detailed immunization history from the officer, including dates of hepatitis B immunizations, previous testing for HIV, HBV, and HCV, tetanus immunization status, and current medications and underlying medical conditions is imperative for proper management of potential pathogen exposure.
REFERENCES
- Henderson Management of needlestick injuries: A House Officer who has a needlestick. JAMA. 2012;307(1):75-84.
- Armstrong K, Gorden R, Santorella Occupational exposure of health care workers (health care workers) to human immunodeficiency virus (HIV): stress reactions and counseling interventions. Soc Work Health Care. 1995;21(3):61-8
- S. Public Health Service. Updated U.S. Public Health Service Guidelines for the Management of Occupational Exposures to HBV, HCV, and HIV and Recommendations for Post exposure Prophylaxis. MMWR Recomm Rep. 2001;50(RR-11):1-52. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5011a1.htm. Accessed August, 2013.
- Kuhar DT, Henderson DK, Struble KA, et Updated US Public Health Service Guidelines for the Man- agement of Occupational Exposures to Human Immunodeficiency Virus and Recommendations for Post- exposure Prophylaxis. Infect Control Hosp Epidemiol. 2013 Sep;34(9):875-892.
- Gen. Stat. sec. 19a-581
Click Here to download the article PDF.
