Published on
Urgent message: Many urgent care centers lack an inventory management process and do not accurately account for their utilization of supplies. Improving how a center manages and accounts for supplies can have a direct impact on the bottom line.
ALAN A. AYERS, MBA, MAcc Practice Velocity
Introduction
A quick and easy way to improve your urgent care center’s profitability may be as close as your supply closet. Many urgent care centers lack defined processes for managing and replenishing medical supplies and their financial statements fail to accurately capture supply inventories and match supply utilization to patient revenues. This results in buying the wrong types of supplies, buying too many supplies, losing supplies to inventory shrinkage, overstating supply expense on the income statement, and understating the value of supplies as an asset on the balance sheet.
Issues With Medical Supply Management in Urgent Care
Medical supplies are items like Band-Aids, syringes, antiseptic, casting material and gauze that are “su stantially consumed” or “materially altered” when used in patient care. In urgent care centers, supplies generally consist of consumables (including injectables and other pharmaceuticals) but they can also include small tools and minor equipment (Table 1).
Some individual supplies (such as suture kits and splints) can be quite costly, but rarely do supplies account for a significant portion of a center’s total expenses. Supplies used are much less extensive than in, say, surgical centers, because most urgent care visits are for low-acuity infections, cold/flu, skin conditions, allergies, etc. Perhaps because medical supplies are viewed as “incidental” to treating patients and are not a major expense category like salaries and rent, many urgent care centers simply “write-off” supplies without further consideration.

Supply Management Starts With a Consensus Formulary
In referring to medical supplies, a stock-keeping unit (SKU) refers to a unique item. In your kitchen cup- board, for instance, “oatmeal” may constitute a single “product” but in a supermarket, each distinct brand, flavor, and box size constitutes a separate “SKU.” This grocery analogy is relevant because—just as any cereal on the shelf may satisfy your morning hunger your urgent care center likely carries multiple SKUs that serve the same clinical purpose. Without an agreed-upon supply “formulary,” if Provider A wants one brand of suture kit and Provider B (who only works weekends) wants a different brand, it’s common for a center to stock both SKUs to appease both providers.
If all of a center’s providers can agree on one SKU for each clinical function—giving fair consideration to quality and price the number of SKUs ordered and stored by the center can be reduced. In addition, by concentrating all orders for a product into one SKU, the center can better take advantage of quantity discounts. To prevent providers and others in the center from ordering whatever they want or need on a whim, however, a formal policy should require that additions or deviations from the formulary be approved by the center’s medical director.
The Need for Formal Supply Management Processes Even when there’s a consensus formulary, many centers lack formal supply management processes to ensure that the “right” quantities of supplies are always on hand. When administrators cannot track how frequently items are used or replenished, they tend to place orders when inventories “appear low” or actually run out. But because running out of a critical supply can impair patient care, it’s likely the center administrator orders and stores far greater quantities than would normally be used in the subsequent weeks or months.
Given that major medical supply houses such as McKesson, PSS World Medical, and Henry Schein offer service level agreements ensuring 48- to 72-hour delivery of nearly any item in their catalogs, a center really has no need to carry more than a couple weeks’ worth of supplies at any given time. Larger inventories increase the risk of shrinkage as supplies expire, spoil, become damaged, or are pilfered. And when these excess quantities start to crowd central storage spaces, supplies end up in exam room cabinets, provider station drawers, and other locations throughout the center further obscuring visibility as to what supplies are on hand.
Electronic Supply Management Systems
A variety of Web-based, supplier-provided and stand- alone inventory management systems have been designed for medical practices can be implemented in an urgent care center. These systems expand upon the use of the SKU identifier to:
- Track current inventory levels against the formulary;
- Track the date supplies were received, number of days on hand, and days until expiration;
- Track supply utilization by category, type, SKU and lot;
- Charge supplies to specific patients, clients or busi- ness units;
- Identify minimum on-hand and trigger reorder quantities;
- Create, track and process requisitions and purchase orders;
- Integrate with supply vendors for electronic ordering and auto-replenishment;
- Reconcile accounts payable invoices to purchase orders and receipts; and
- Create inventory reports to facilitate physical
Electronic inventory systems are most effective when integrated with bar code technology. Using a handheld device, staff “scans” the bar codes on individual items as they’re consumed in patient care (or on boxes as they’re opened or removed from the storage closet). The system then electronically updates inventory records, facilitating on-demand reports of supplies on hand and those used during a reporting period. Periodic inventory can be facilitated using the bar code scanner and system reports. The system can even indicate when quantities fall to preset “reorder” levels. More sophisticated systems can automatically create a purchase order and submit an electronic order to the supply vendor for fulfillment.
Not all urgent care centers will want to computerize their ordering and inventory management processes. But applying simple internal control procedures and routine authorizations for expenditures will still significantly help in managing supply costs. When an inventory system is implemented, quantities in use and on hand tend to be consistent and, therefore, accurate records lead to generation of a more consistent month- over-month supply expense on the income statement; reduction in overstock, waste and spoilage; and more efficient use of storage space.
Account for Supply Utilization
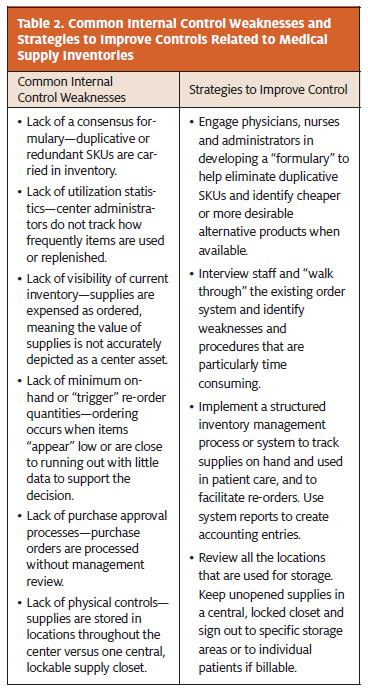
From an accounting standpoint, an urgent care center’s management is responsible for the accurate presentation of financial statements prepared for use by creditors and investors under Generally Accepted Accounting Princi- ples (GAAP). Accurately representing Supply Expense on the Income Statement and the value of Supply Inven- tory on the Balance Sheet requires adequate financial controls, as illustrated in Table 2.
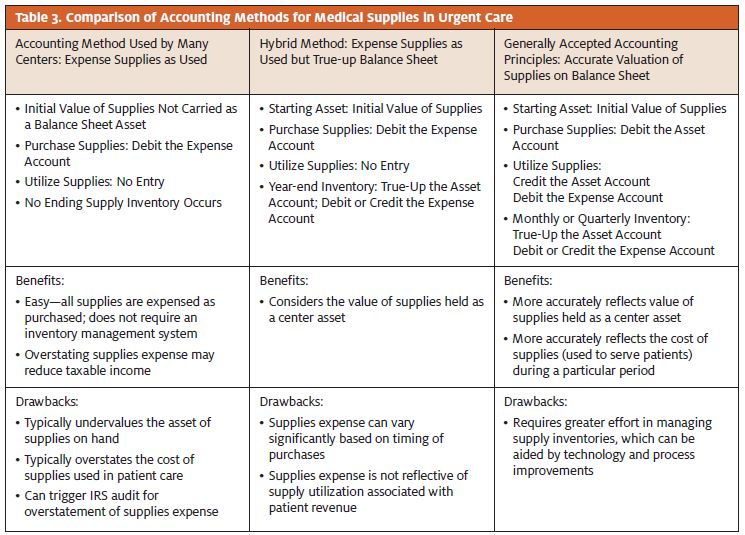
Often urgent care centers do not maintain accurate supply inventories on their books because they expense all supplies at the time of purchase. The issue with this illustrated by Table 3—is that an asset worth up to $50,000 (in aggregate) is hidden away in cabinets, drawers, and under sinks while the Balance Sheet understates the value of owners’ equity in the business.
Moreover, the common practice of expensing all supplies upon purchase violates accounting principles that call for revenue and expenses to be matched during the same period each is incurred. In any given month that a large supply order is processed, supplies expense as a percent of patient revenue may climb, leading to incorrect conclusions being drawn from the income statement. Likewise, a center could improve its profitability in a given month by just not placing any supply orders.
As illustrated in Table 3, center accounting for supplies could be improved by carrying a beginning supply inventory on the balance sheet, continuing to expense supplies as used, and doing a periodic “true-up” based on a physical inventory count. But the best alter- native is to record purchases in the inventory (asset) account and make a periodic journal entry (weekly or monthly) to expense sup- plies that are used. The availability of data from an inventory management system facilitates this routine. In addition, a physical inventory will be matched to the account balances and any differences analyzed. With supply expense more reflective of utilization, a center operator can more effectively identify trends, including changes in supply costs.
Payor Reimbursement for Medical Supplies
In general, urgent care centers are not specifically reimbursed for supplies used in the ordinary treatment of patients. This is particularly true when a center has contracts that pay a “flat fee” or “global rate” per visit. But some fee-for-service contracts do reimburse some supplies—particularly supplies used in procedures like casting and suturing. Thus, center administrators should understand which supplies are reimbursed by which payors using which codes. When supplies are reimbursable, a process should be in place to accurately capture supply utilization on the patient’s charge ticket. Providers, medical assistants, and charge entry staff also need to be educated as to which payors reimburse which supplies to ensure chart documentation such that the center receives its full reimbursement.
Conclusion
Improving your urgent care center’s medical supply management processes can have a direct impact on its financials by better tying supply utilization expense to patient revenue and by better reflecting supplies on hand as an asset of the center. Effective supply management in urgent care entails establishing a formulary, implementing processes related to the storage and replenishment of supplies, capturing supply utilization and shrink, and establishing proper accounting practices.
