Published on
Download the article PDF: The Impact Of An Urgent Care Point Of Care Ultrasound Program On Patient Transfers To The Emergency Department
Urgent Message: Training urgent care providers to use point-of-care ultrasound resulted in fewer patient transfers to the emergency department for soft tissue/musculoskeletal and first-trimester pregnancy complaints, while also streamlining care in this single-center program.
Keywords: point-of-care ultrasound; urgent care; emergency department transfer; soft tissue infection; musculoskeletal complaints; first-trimester pregnancy
Lindsey E. Fish, MD, FCUCM; Genie Roosevelt, MD; Amanda G. Toney, MD
Abstract
Introduction: The use of point-of-care ultrasound (POCUS) is expanding into multiple clinical areas as it has been shown to improve patient outcomes and satisfaction, and decrease length of stay and patient costs. However, very limited research has been performed on the impact of POCUS implementation in the urgent care (UC) setting. We aimed to compare the transfer rate to the emergency department (ED) for ultrasound imaging for patients presenting to the UC with soft tissue/musculoskeletal (ST/MSK) and first-trimester-pregnancy-related complaints prior to and after a POCUS educational intervention.
Methods: UC providers from a single clinic participated in a 1-day POCUS training course focused on aorta, renal, ST/MSK, and transabdominal first-trimester pregnancy ultrasound studies. Using retrospective electronic record chart review, all patients who presented to the UC with a ST/MSK or first-trimester-pregnancy complaint were identified 10 months prior to and following POCUS training. Categorical variables were evaluated with the chi-square test, and relative risk ratios (RR) with 95% confidence intervals (CI) were calculated.
Results: For ST/MSK complaints, prior to the POCUS training course, 5.1% of patients were transferred compared to 2.2% after the course. The risk of transfer was 2.30 times higher (RR) (95% CI 1.27–4.14, p=0.0006) before the course compared with after it, which was statistically significant. For first-trimester pregnancy complaints, prior to the POCUS course, 28% of patients were transferred compared to 20% after the course. The risk of transfer was 1.42 times higher (RR) (95% CI 0.99–2.05, p=0.06) before the course compared with after it, which was not statistically significant.
Conclusion: In this single urgent care setting, teaching UC providers POCUS skills resulted in a decreased percentage of patient transfers to the ED for ST/MSK and first-trimester pregnancy complaints, thus streamlining patient care.
Introduction
The use of point-of-care ultrasound (POCUS) is expanding into multiple areas of medicine, including emergency departments (ED), outpatient clinics, and inpatient units as it has been shown to improve patient outcomes and satisfaction while also decreasing length of stay and patient costs.1-7 The American College of Emergency Physicians has an extensive policy statement regarding emergency, point-of-care, and clinical ultrasound guidelines for this expanding field.8 Urgent care (UC) clinics are emerging as a new site for POCUS application, which may facilitate patient care. As with any new area of medicine, there are several challenges for UC in implementing POCUS.9 Specifically, it appears that no curricula or guidelines exist, and very limited research has been performed on the impact of POCUS implementation in the UC setting. We hypothesized that the implementation of a POCUS training course and quality assurance (QA) program for UC providers (physicians, nurse practitioners, and physician assistants) would allow them to make better informed clinical decisions, thus decreasing transfers to the ED. The objectives of the POCUS training course for this UC were to expedite patient care, decrease the cost of care for the patient by decreasing ED transfers (ie, avoiding 2 encounters for 1 complaint), and to decrease patient volume at the ED.
The Federico F. Peña Southwest Urgent Care Clinic opened in 2016 as a community-health-based UC clinic affiliated with Denver Health and Hospital (Denver, Colorado), a safety-net healthcare institution. The aim of the clinic is to provide diagnostic and management services to patients in their local community regardless of age, complaint, language, race/ethnicity, insurance status, or ability to pay. Daily clinic operations are performed by physicians, nurse practitioners, physician assistants, registered nurses, medical assistants, and patient access specialists. This moderate/advanced UC clinic provides onsite laboratory testing, x-ray, intravenous fluids, and clinic administered medications. However, it does not provide consultative ultrasound or computerized tomography (CT), cardiopulmonary monitoring, advanced airway support, or cardiac resuscitation. At the time of this program, this UC clinic provided over 25,000 visits a year to a primarily underserved population including patients covered by Medicare/Medicaid (65%), uninsured (15%), and sliding-scale self-pay (12%)—as well as Spanish-speaking patients (35%) and patients who speak other languages (5%). The transfer rate of patients to the hospital for a higher level of care was less than 5%. Transfers are performed via private vehicle, nonemergent ambulance, and emergent ambulance. The majority of transfers are referred to the Denver Health ED, which is 3 miles away from Peña Urgent Care Clinic, however, there are transfers to other local hospitals as well.
Our study objective was to compare the transfer rate to the ED for ultrasound imaging for patients presenting to the UC with soft tissue/musculoskeletal (ST/MSK) and first-trimester-pregnancy-related complaints prior to and after a POCUS training course.
Methods
All UC providers (10) from the clinic participated in a 1-day POCUS training course on March 4, 2017. The training focused on 4 applications: aorta; renal; ST/MSK; and transabdominal first-trimester pregnancy ultrasound studies. The course was presented by the Denver Health Director of Pediatric Emergency Ultrasound—who is also the Director of the Pediatric Emergency Ultrasound Fellowship—along with several Denver Health emergency ultrasound fellows. The coursework included an overview of POCUS and its broad uses, instruction on the practical use of the specific ultrasound machine available in the UC, and standardized hands-on practice studies on multiple patients. Following the course, providers were evaluated on their clinic-performed ultrasound images and interpretations, which were reviewed for quality assurance by POCUS experts, with a goal of 25 scans for each of the 4 applications, aligned with hospital credentialing requirements.
Using retrospective electronic record chart review, all patients who presented to the UC with a ST/MSK or first-trimester pregnancy complaint were identified using ICD-10 diagnosis codes 10 months prior to POCUS training and 10 months following POCUS training. After an extensive search of all applicable ICD-10 codes, the codes utilized for ST/MSK complaints were L02.X, L03.X, L05.X, L08.9, M79.5, R19.XX, R22.XX, and T14.8XXA. The ICD-10 codes utilized for first-trimester pregnancy complaints were O02.X, O03.X, O20.X, O26.89X, O46.X, O99.89X, Z33.X, Z34.X, and Z3A.XX. The number of transfers to the ED for each of these complaints was identified from the UC transfer log—a manual log that records each transfer, including patient identification, complaint, reason for transfer, and method of transport.
Continuous variables with normal distributions were analyzed with a Student’s t test. Continuous variables with non-normal distributions were analyzed with a Mann-Whitney U test. Categorical variables were evaluated with the chi-square test, and relative risk (RR) with 95% confidence intervals (CI) were calculated. A p value of £0.05 was considered statistically significant. Analyses were performed using IBM SPSS Statistics, Version 28 (Armonk, New York).
Results
Soft Tissue/Musculoskeletal
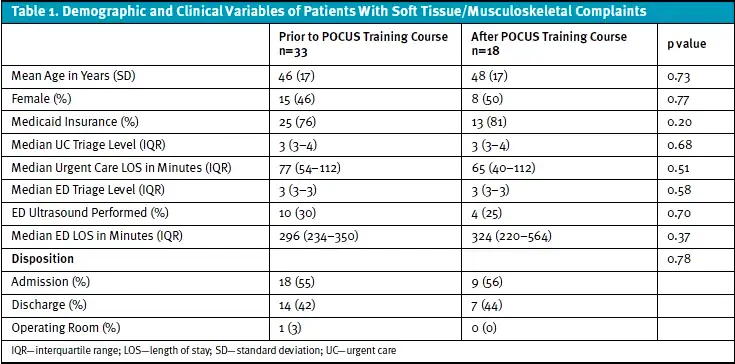
During the time period before the training course, 40 (5.1%) out of 780 patients with ST/MSK complaints were transferred to the ED from the UC. Seven of those patients were excluded (5 patients were directly admitted without an ED visit; 2 patients did not present to the ED), leaving 33 patients for analysis. After the training course, 19 (2.2%) out of 871 patients with ST/MSK complaints were transferred from the UC. One of those patients was excluded (transferred to a different facility), leaving 18 patients for analysis. The patients in the precourse time period and postcourse time period had similar demographic and clinical characteristics (Table 1). The risk of ED transfer was 2.30 times (RR) higher (95% CI 1.27–4.14, p=0.0006) in the time before the training course compared with after, which was statistically significant.
First-Trimester Pregnancy
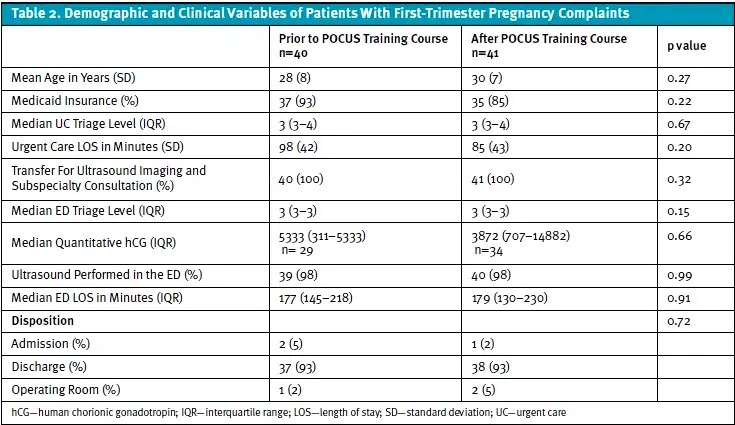
During the precourse time period, 45 (28%) out of 158 patients with first-trimester pregnancy complaints were transferred from the UC. Five of those patients were excluded (3 were transferred directly to the obstetrics service; 1 was transferred to another facility due to insurance; 1 did not present to the ED), leaving 40 patients for further analysis. After the course, 43 (20%) out of 215 patients with first-trimester pregnancy complaints were transferred from the UC. Two patients were excluded (1 was transferred directly to the obstetrics service; 1 was transferred to another ED), leaving 41 patients for further analysis. The patients in the precourse time period and postcourse time period had similar demographic and clinical characteristics (Table 2). The risk of transfer was 1.42 times higher (RR) (95% CI 0.99–2.05, p=0.06) before the training course compared with after, which was not statistically significant.
Discussion
We were able to successfully create and implement a POCUS training course and QA program for a UC setting. To our knowledge, these are the first results of such a program to be published in the literature. Although we focused on 4 applications initially (aorta, renal, ST/MSK, and first-trimester pregnancy exam), the ST/MSK and first-trimester pregnancy applications were performed most often in the clinic. Furthermore, QA, including image and interpretation review and feedback, was necessary to develop and maintain ultrasound skills. The ongoing QA program not only provides feedback to the providers but also serves as a potential pathway for UC POCUS credentialing.
The UC POCUS program was effective and resulted in a statistically significant 2-fold decrease in ED transfers for ST/MSK related complaints and a trend toward decreases in ED transfer for first-trimester-pregnancy complaints, thus expediting patient care.
While few studies from the United States assess the impact of POCUS on transfer rate to a higher level of care, a study from New Zealand reported that POCUS use by generalists in 6 rural hospitals decreased the rate of admission and transfer to an urban referral hospital by 4%.10 The rural hospitals included were similar to UC clinics in the United States as only half had consultative ultrasound available during work hours, and 1 had computed tomography available. Another group of physicians working at a remote multiday music festival in British Columbia, Canada, found that POCUS use reduced ambulance transport off-site by 32%.11 Further studies are needed to assess the impact of POCUS use on transfer rate and to assess for any potential patient harm if transfer did not occur.
The addition of POCUS in the UC clinic was not associated with a noted increase in length of stay (LOS) of the urgent care visit. Although not directly measured in this study, we can infer that by decreasing the transfer rate, we were able to decrease LOS for the entirety of the patient experience. Given the decrease in patient transfers, it is reasonable to assume patients spent less time in transfer, waiting in the ED waiting room, and receiving care in the ED. Several studies have reported that the use of POCUS decreased LOS and expedited care in the ED and critical care settings.12-17 LOS has been reduced for several patient groups including those with the following complaints: pelvic,13,17 early pregnancy,16 soft tissue,15 appendicitis,14 and shock.12 POCUS use in UC appears to have the ability to significantly improve patient satisfaction by reducing the time spent receiving care.
Furthermore, we can reasonably assume that there was a reduction in costs for the patients because fewer patients were transferred to the ED for additional care. POCUS has also been shown in the literature to decrease patient costs.1,5,18 For example, a 2019 study in a community ED in the United States found that POCUS use reduced costs by $1,134.31 for privately insured patients, $2,826.31 for out-of-network or uninsured patients, and $181.63 for Medicare and Medicaid patients by avoiding additional testing.19 POCUS may also offer an additional source of revenue for a UC clinic that is able to bill for the procedure.
Our study also suggests, given the decrease in transfer rate for patients with ST/MSK and first-trimester pregnancy complaints, decreased burden on the ED in terms of patient volume and utilization of resources. A reduction in transfer rate infers fewer ambulance transports, a lower ED volume, and a decrease in utilization of consultative radiology resources. A recent randomized controlled trial comparing lung POCUS with chest x-ray (CXR) in children suspected of having pneumonia in an ED showed a reduction in CXR use when POCUS was available.20 The patients in the control arm had a POCUS exam and CXR. The investigational arm included patients who received a POCUS exam but the CXR was optional. Investigators found a 38% reduction in CXR use in the investigational arm, which reduced radiation exposure and cost. We did not directly assess ED resource utilization in our study, and future studies should explore these outcomes.
There are several limitations of our study including that it is a single-center study, which limits its generalizability to other urgent care centers. The study is retrospective, therefore, important variables may be absent, inconsistently recorded, or inaccurate in the analyzed data, and there may be other confounding factors. We did not directly study UC length-of-stay, the rate of consultative radiology orders, patient costs, and patient return visits, which are important outcomes and should be included in future studies.
Conclusion
In this single urgent care setting, teaching UC providers POCUS skills resulted in a decreased percentage of patient transfers to the ED for ST/MSK and first-trimester pregnancy complaints, thus streamlining the care of the patient.
Manuscript submitted November 13, 2025; accepted May 6, 2026.
References
- 1Calvert N, Hind D, McWilliams RG, Thomas SM, Beverley C, Davidson A. The effectiveness and cost-effectiveness of ultrasound locating devices for central venous access: a systematic review and economic evaluation. Health Technol Assess. 2003;7(12):1-84.
- Colli A, Prati D, Fraquelli M, et al. The use of a pocket-sized ultrasound device improves physical examination: results of an in- and outpatient cohort study. PLoS One. 2015;10(3):e0122181.
- Gordon CE, Feller-Kopman D, Balk EM, Smetana GW. Pneumothorax following thoracentesis: a systematic review and meta-analysis. Arch Intern Med. 2010;170(4):332-339.
- Howard ZD, Noble VE, Marill KA, et al. Bedside ultrasound maximizes patient satisfaction. J Emerg Med. 2014;46(1):46-53.
- Parker L, Nazarian LN, Carrino JA, et al. Musculoskeletal imaging: Medicare use, costs, and potential for cost substitution. J Am Coll Radiol. 2008;5(3):182-188.
- Smith-Bindman R, Aubin C, Bailitz J, et al. Ultrasonography versus computed tomography for suspected nephrolithiasis. N Engl J Med. 2014;371(12):1100-1110.
- Marin JR, Abo AM, Arroyo AC, et al. Pediatric emergency medicine point-of-care ultrasound: summary of the evidence. Crit Ultrasound J. 2016;8(1):16.
- Ultrasound Guidelines: Emergency, Point-of-Care and Clinical Ultrasound Guidelines in Medicine. Ann Emerg Med. 2017;69(5):e27-e54.
- Hicks J. Point Of Care Ultrasound (POCUS) In Urgent Care. J Urgent Care Med. Published October 30, 2018. Accessed November 1, 2025. https://www.jucm.com/point-of-care-ultrasound-pocus-in-urgent-care/.
- Nixon G, Blattner K, Koroheke-Rogers M, et al. Point-of-care ultrasound in rural New Zealand: Safety, quality and impact on patient management. Aust J Rural Health. 2018;26(5):342-349.
- Prager R, Sedgwick C, Lund A, et al. Prospective Evaluation of Point-of-Care Ultrasound at a Remote, Multi-Day Music Festival. Prehosp Disaster Med. 2018;33(5):484-489.
- Chen Z, Hong Y, Dai J, Xing L. Incorporation of point-of-care ultrasound into morning round is associated with improvement in clinical outcomes in critically ill patients with sepsis. J Clin Anesth. 2018;48:62-66.
- Chiem AT, Chan CH, Ibrahim DY, et al. Pelvic ultrasonography and length of stay in the ED: an observational study. Am J Emerg Med. 2014;32(12):1464-1469.
- Lalande E, Parent MC. Towards evidence-based emergency medicine: best BETs from the Manchester Royal Infirmary. BET 1: Impact of point-of-care ultrasound on length of stay for paediatric appendicitis. Emerg Med J. 2015;32(7):574-575.
- Lin MJ, Neuman M, Rempell R, Monuteaux M, Levy J. Point-of-Care Ultrasound is Associated With Decreased Length of Stay in Children Presenting to the Emergency Department With Soft Tissue Infection. J Emerg Med. 2018;54(1):96-101.
- Morgan BB, Kao A, Trent SA, et al. Effect of Emergency Physician-Performed Point-of-Care Ultrasound and Radiology Department-Performed Ultrasound Examinations on the Emergency Department Length of Stay Among Pregnant Women at Less Than 20 Weeks’ Gestation. J Ultrasound Med. 2018;37(11):2497-2505.
- Shih CH. Effect of emergency physician-performed pelvic sonography on length of stay in the emergency department. Ann Emerg Med. 1997;29(3):348-351; discussion 352.
- Mercaldi CJ, Lanes SF. Ultrasound guidance decreases complications and improves the cost of care among patients undergoing thoracentesis and paracentesis. Chest. 2013;143(2):532-538.
- Van Schaik GWW, Van Schaik KD, Murphy MC. Point-of-Care Ultrasonography (POCUS) in a Community Emergency Department: An Analysis of Decision Making and Cost Savings Associated With POCUS. J Ultrasound Med. 2019;38(8):2133-2140.
- Jones BP, Tay ET, Elikashvili I, et al. Feasibility and Safety of Substituting Lung Ultrasonography for Chest Radiography When Diagnosing Pneumonia in Children: A Randomized Controlled Trial. Chest. 2016;150(1):131-138.
Author Affiliations: Lindsey E. Fish, MD, FCUCM, Division of Urgent Care, Ambulatory Care Services, Denver Health and Hospital, Denver, Colorado; Division of General Internal Medicine, Department of Medicine, University of Colorado School of Medicine, Aurora, Colorado; The Journal of Urgent Care Medicine. Genie Roosevelt MD, Department of Emergency Medicine, Denver Health and Hospital, Denver, Colorado; Department of Emergency Medicine, University of Colorado School of Medicine, Aurora, Colorado. Amanda G. Toney, MD, Department of Emergency Medicine, Denver Health and Hospital, Denver, Colorado; Department of Emergency Medicine, University of Colorado School of Medicine, Aurora, Colorado. Authors have no relevant financial relationships with any ineligible companies.
