Published on
Urgent message: In patients with chest pain, check chest films carefully to avoid missing an uncommon diagnosis.
Joseph Toscano, MD
Introduction
The traditional differential diagnosis for chest pain includes spontaneous pneumothorax. Chest x-ray is necessary for confirming the diagnosis, and sometimes the findings can be subtle. As in dealing with any infrequently encountered condition, clinicians should consider the diagnosis and closely examine every chest film they order to avoid missing this uncommon diagnosis.
Case Presentation
TE is a 36-year-old female who developed right-sided chest pain while at rest earlier that same day. She had a constant sensation of soreness in her anterior and apical right chest, with periods of increased, sharper pain with deep inspiration. TE had mild shortness of breath and denied trauma, recent illness, fever, or cough. She otherwise felt well and noted no prior history of similar problems. Her past medical history was negative for asthma, other pulmonary problems or medical conditions. She took oral contraceptives, but no other medications and had no allergies. She did not smoke or use illicit drugs.
Observation and Findings
Evaluation of the patient revealed the following:
- Temp: 98.9°F
- P: 84
- R: 22
- BP 115/74
- O2 Sat: 98% RA
- Gen: WD, WN, no Marfanoid features, mild distress to intermittent sharp pain
- HEENT: No signs of trauma, mass, infection, edema
- Neck: Supple, nontender, no lymphadenopathy, no JVD
- Chest: No visible abnormalities or tenderness
- Lungs: Decreased breath sounds, no wheezes or rales
- CV: RRR, no murmur or gallop, palpably symmetric radial pulses
- Abd: Nontender, no distension
- Neuro: Normal MS; no abnormalities of strength, sensation, coordination, gait
Radiology results revealed the following:
Chest x-ray (Figure 1): Initially read by the urgent care clinician as showing a normal cardiac and mediastinal silhouette, clear lung fields, no effusions.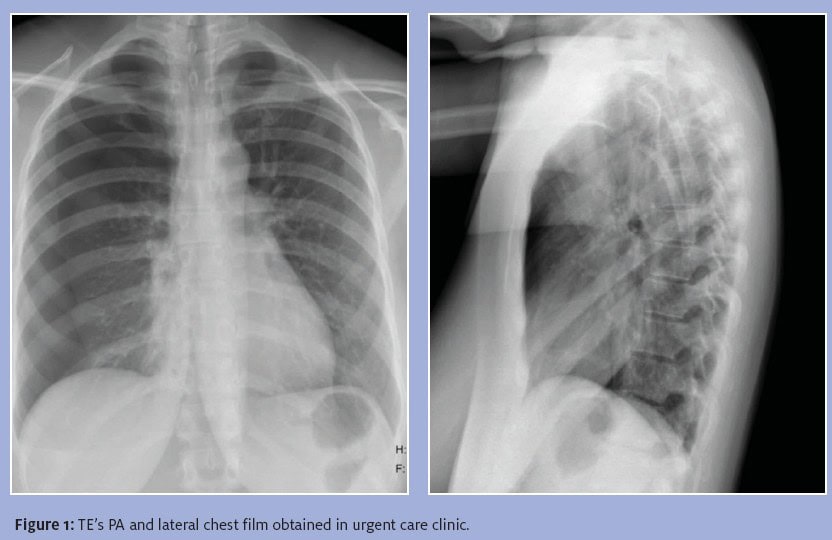
Course and Treatment
The patient was diagnosed with pleurisy and prescribed ibuprofen and hydrocodone/APAP, and primary MD follow-up was recommended for 2-3 days later. A radiologist over-read the film later the same day and diagnosed a right pneumothorax. The patient was contacted and instructed to go to the emergency department, where a chest tube was placed, with successful re-expansion of her lung. The patient was admitted, her chest tube was discontinued after 4 days, and she was discharged. A CT scan of the chest showed no bullous changes or other pulmonary parenchymal abnormality.
Discussion
Pneumothorax results from the passage of air into the normally gasless pleural space, either through a defect externally in the chest wall or internally in the pulmonary parenchyma or tracheobronchial tree. The majority of pneumothoraces are due to trauma, but come do occur spontaneously, at an annual rate of about 0.007 – 0.018% in men and a rate of about one-third to one-fifth of that in women. Recurrence rates can be as high as 35%. The typical patient who develops spontaneous pneumothorax is a tall, thin male smoker, so TE is an unusual case.
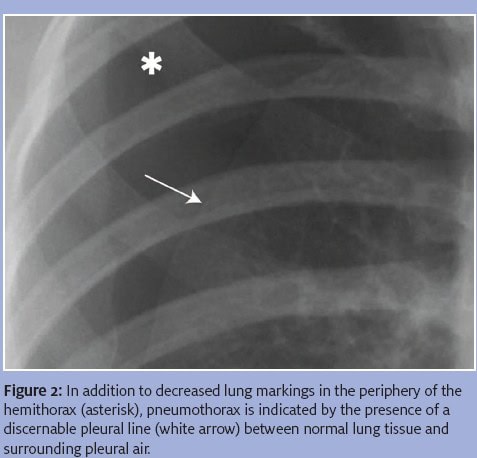
Typical symptoms include dyspnea and chest discomfort, which may be sharp or achy. Small pneumothoraces (<15% of the hemithoracic volume) may be difficult to detect on physical exam. Although CT scanning is more sensitive than plain films, clinically significant pneumothoraces should be visible on chest x-ray. In addition to a lack of normal pulmonary markings in the periphery of the hemithorax, finding a “pleural line” (Figure 2) increases the specificity of the diagnosis. Since the advent of digital radiography, there are some data to suggest that diagnostic accuracy is lower at resolutions near 1.25 line pairs per millimeter (lp/mm), so those using digital technique at their clinics should ensure system settings of at least 2.5 lp/mm. Reliable techniques for diagnosing pneumothorax using bedside ultrasound have been developed for situations in which rapid diagnosis is important. Otherwise, though it is arguable whether every patient with chest pain requires a chest x -ray (and ECG), this diagnosis cannot be confirmed without it.
Treatment includes evacuation of air from the pleural space through any of a variety of methods, some of which (such as a small-gauge catheter and Heimlich valve) may be performed in an outpatient setting. Further work-up of patients with spontaneous pneumothoraces includes chest CT without contrast to identify pulmonary parenchymal abnormalities such as bullae that predispose to recurrence and can be corrected surgically.
Simple pneumothoraces are not life threatening, though a rare complication includes development of a tension pneumothorax, which occurs when a flutter-valve effect develops in the chest wall or pulmonary defect. This permits air to pass only into the pleural space, allowing positive pressure to develop there, compressing to the heart, causing hemodynamic instability. This requires immediate needle thoracostomy.
Conclusion
Spontaneous pneumothorax is a rare cause of chest discomfort or dyspnea and patients with it can present to the urgent care clinic. Correct diagnosis requires careful attention to chest x-ray findings.
References
- Sahn SA, Heffner JE. Spontaneous pneumothorax. N Engl J Med. 2000; 342(12): 868-874.
- Silva DR, Schuch SJ, Dalcin P. Posteranterior chest xray for the diagnosis of pneumothorax: methods, usage, and resolution. Reports in Medical Imaging. 2010; 3: 29-34
- Wakai AP. Spontaneous pneumothorax. Clin Evid (Online) 2008; 2008: 1505. Accessed June 16, 2011.
