Published on
Urgent message: Patients with chest pain/acute coronary syndrome often present in outpatient medical settings—including urgent care centers—not designed to treat life-threatening conditions. Exclusive new data suggest that urgent care centers need to be integrated into pre-hospital cardiovascular care pathways.
JASON T. WEINGART, MD, THOMAS P. CARRIGAN, MD, MHSA, LEE RESNICK, MD, DANIEL ELLENBERGER, BS, DANIEL I. SIMON, MD, and RICHARD A. JOSEPHSON, MS, MD
Emergency medical services and hospital-based emergency departments (EDs) are typically incorporated into systems of care for patients with chest pain/acute coronary syndrome (ACS) but the role of free-standing urgent care centers (UCCs) in the evaluation and treatment of such patients is underappreciated. Between May 21, 2008 and June 9, 2009, 500 patients presented to any 1 of 5 UCCs in the greater Cleveland area with chest pain/possible ACS. Of those patients, 10.4% were troponin-positive on presentation. Detailed follow-up is presented for the 155 patients admitted to the university medical center. Eighteen (11.6%) of those admitted were high acuity: 2 with ST elevation myocardial infarction (STEMI), 9 with non-ST elevation myocardial infarction (NSTEMI), 5 additional patients underwent urgent percutaneous coronary intervention (PCI) for unstable angina, 1 with pulmonary embolus, and 1 aortic dissection. UCCs provide pre-hospital access to patients presenting with chest pain/ACS and need to be integrated into cardiovascular care pathways.
 Considerable public and professional education is directed at the importance and benefit of early and rapid evaluation of chest pain and related symptoms that may be indicative of ACS.1 Many health care systems and geographic regions, including our own, have organized a regional approach to patients with possible ACS.2,3 These efforts typically focus on improving efficiencies between a patient’s first medical contact via emergency medical systems or EDs and definitive treatment.4-8 Existing data demonstrate that improved treatment times and efficiencies offer a survival advantage, whereas delays can increase mortality rates.8,9 Our region has many hospital-based EDs and also a network of free-standing urgent care centers (UCCs). Nationally, there are estimated to be 4,600 EDs and more than 9,000 UCCs, which are a growing provider of outpatient services.10 The Urgent Care Association defines UCCs as walk-in medical clinics designed to treat non-life threatening ill- nesses and injuries, usually at lower cost and with shorter service times than EDs. These centers are staffed by a variety of physicians, many of whom are not board-certified in Emergency Medicine or Cardiovascular Disease, and thus, may not have received the same level of training regarding the diagnosis and treatment of ACS as these specialists. Furthermore, UCCs often have neither the diagnos- tic testing infrastructure nor the broad array of drugs to treat patients that are available in hospital-based EDs.
Considerable public and professional education is directed at the importance and benefit of early and rapid evaluation of chest pain and related symptoms that may be indicative of ACS.1 Many health care systems and geographic regions, including our own, have organized a regional approach to patients with possible ACS.2,3 These efforts typically focus on improving efficiencies between a patient’s first medical contact via emergency medical systems or EDs and definitive treatment.4-8 Existing data demonstrate that improved treatment times and efficiencies offer a survival advantage, whereas delays can increase mortality rates.8,9 Our region has many hospital-based EDs and also a network of free-standing urgent care centers (UCCs). Nationally, there are estimated to be 4,600 EDs and more than 9,000 UCCs, which are a growing provider of outpatient services.10 The Urgent Care Association defines UCCs as walk-in medical clinics designed to treat non-life threatening ill- nesses and injuries, usually at lower cost and with shorter service times than EDs. These centers are staffed by a variety of physicians, many of whom are not board-certified in Emergency Medicine or Cardiovascular Disease, and thus, may not have received the same level of training regarding the diagnosis and treatment of ACS as these specialists. Furthermore, UCCs often have neither the diagnos- tic testing infrastructure nor the broad array of drugs to treat patients that are available in hospital-based EDs.
Despite the availability of hospital-based EDs and public education instructing patients to use UCCs for non-emergent/non-life-threatening symptoms, we observed that patients with ACS often present to UCCs. The purpose of this study was to examine this under-recognized and important patient population and evaluate the safety and efficacy of combining clinical decision-making tools with a single point-of-care troponin measurement to more accurately identify ACS while decreasing unnecessary admissions, transfers, and utilization for those at lower risk. Currently there exists no guideline to sup- port patient assessment and triage of the ambulatory outpatient with possible ACS. Without effective means for triaging these patients, the provider is left with few practical options. The decision to transfer all of these patients to tertiary care centers results in a significant financial and psychological burden despite the low incidence of disease. However, triage by history and risk factors alone is fraught with low sensitivity and high risk. The medical liability issues pertaining to missed myocardial infarction have made it increasingly difficult to evaluate these patients in the outpatient setting without more sensitive and efficient methods of evaluation.
Methods
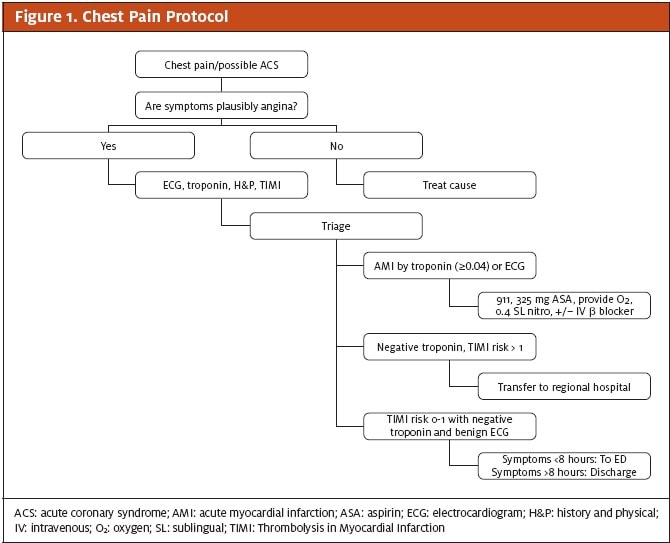
We analyzed 500 consecutive patients presenting with signs or symptoms suggestive of ACS who presented to any 1 of 5 UCCs in the University Hospitals Health System from May 21, 2008 to June 9, 2009. These 5 UCCs were geographically dispersed but administratively linked to a multi-hospital health system that included a university-affiliated quaternary care teaching hospital. Data were recorded prospectively by clinical staff at each UCC. All patients underwent expedited protocol- guided evaluation, including focused history and physical exam, electrocardiogram (ECG), point-of-care troponin (iSTAT, Abbot Labs) and calculation of thrombolysis in myocardial infarction (TIMI) risk score,11 Per protocol, patients with acutely abnormal ECG, elevated troponin I or a TIMI risk score >1, or a presentation of less than 8 hours since the onset of symptoms were referred to a hospital for evaluation. Additional patients were referred at the discretion of the treating physician (Figure 1). Referral to a particular area hospital, including our health system’s quaternary care medical center, was based largely on geographical and/or insurance considerations.
Ba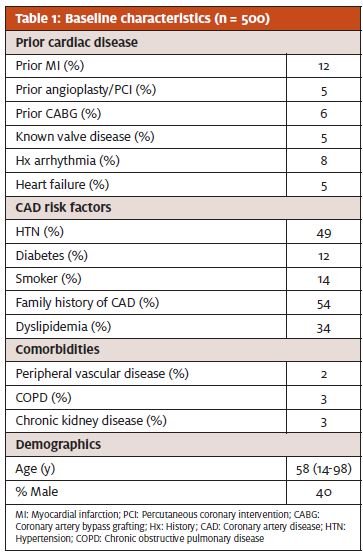 seline characteristics, including chief complaint, medical history, coronary risk factors, UCC diagnosis, and patient disposition, were obtained. Medical history and coronary risk factors were determined by physician documentation in the medical record. Final diagnosis was obtained by review of inpatient medical records for 155 patients transferred and admitted to University Hospitals Case Medical Center. Eight patients referred for hospital transfer declined.
seline characteristics, including chief complaint, medical history, coronary risk factors, UCC diagnosis, and patient disposition, were obtained. Medical history and coronary risk factors were determined by physician documentation in the medical record. Final diagnosis was obtained by review of inpatient medical records for 155 patients transferred and admitted to University Hospitals Case Medical Center. Eight patients referred for hospital transfer declined.
Results
The demographic information and characteristics of the study population are summarized in Table 1. The average age was age 58 and 60% of the population was female. The patient age distribution is summarized in Figure 2. Many patients had known coronary artery disease, including 12% with prior myocardial infarction, 6% with prior coronary artery bypass graft, and 5% with prior PCI. Overall, the majority of patients had at least 1 major coronary artery disease (CAD) risk factor, including 49% with hypertension, 14% with cigarette smoking, and 12% with diabetes.
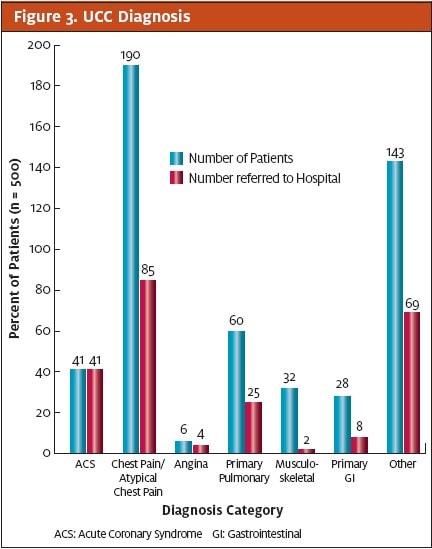
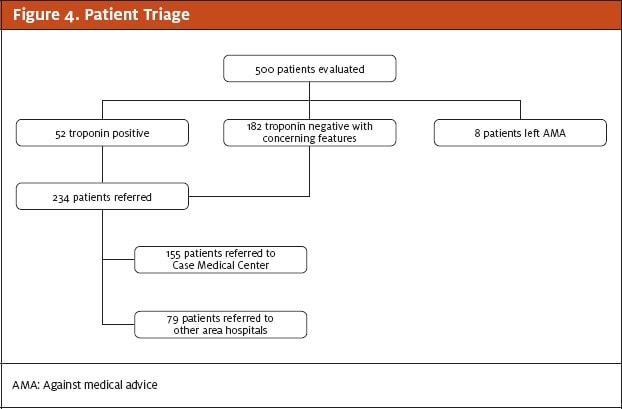
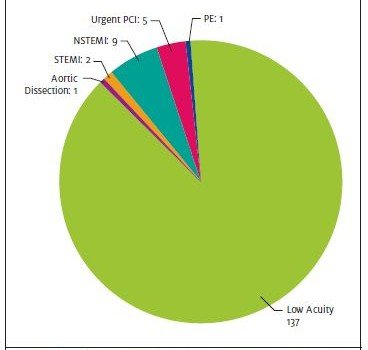
Of the 500 patients evaluated 52 (10.4%) were troponin-positive on presentation. All 52 troponin-positive patients and an additional 182 (36.4%) of patients who were initially troponin-negative but had a concerning clinical presentation as assessed by the UCC physician, often in telephone consultation with the attending cardiologist at the quaternary medical center, were referred for further evaluation and treatment (Figures 3 and 4). Of the 155 patients referred to the quaternary medical center, 18 (11.6%) had serious and potentially life- threatening disease: 2 with STEMI, 9 with NSTEMI, 5 unstable angina patients requiring urgent PCI, 1 pulmonary embolism, and 1 aortic dissection. These results are summarized in Figure 5.
Discussion
Chest pain and related symptoms are one of the most common reasons patients present to an ED in the United States each year. The 2006 Centers for Disease Control Emergency Department Summary reports that 6.4 million (5.4%) of the estimated 119 million ED visits in 2006 were for chest pain or related symptoms.12 Despite public and professional education programs designed to alert patients to the signs and symptoms of ACS, and to seek care via emergency medical systems, our data illustrate that patients frequently present to UCCs with chest pain. The actual number of UCC patients is clearly large and significant and optimization of their care is a worthwhile goal. By way of comparison, the quaternary care medical center in our study that admitted 155 patients directly from the UCC system had 2,406 patients admitted with similar presenting symptoms from the hospital-based ED during that same time period (403 with acute myocardial infarction, 333 with angina pectoris, and 1,670 with chest pain).
 Previous studies have suggested that community education programs on the signs and symptoms of a heart attack may improve resource utilization and patient outcomes,13 yet recent evidence from a randomized, con- trolled trial suggests that even in a population of patients with known coronary disease, an intensive effort of education and counseling does not result in the reduction of pre-hospital delays.14 When taken in conjunction with our data, in a population of patients predominately without a prior history of CAD, public education pro- grams on a local or national level are likely to be expensive and suboptimal. Therefore, as health systems begin to regionalize their ACS care, integration with UCCs should be strongly considered.
Previous studies have suggested that community education programs on the signs and symptoms of a heart attack may improve resource utilization and patient outcomes,13 yet recent evidence from a randomized, con- trolled trial suggests that even in a population of patients with known coronary disease, an intensive effort of education and counseling does not result in the reduction of pre-hospital delays.14 When taken in conjunction with our data, in a population of patients predominately without a prior history of CAD, public education pro- grams on a local or national level are likely to be expensive and suboptimal. Therefore, as health systems begin to regionalize their ACS care, integration with UCCs should be strongly considered.
In our study of 500 consecutive patients in a typical US metropolitan region over a 1- year period presenting to an UCC with a clinical picture suggestive of ACS, patients with potentially life-threatening disease were frequently encountered. Further- more, more than 1 in 10 of these patients required true emergent medical attention and therapy. These patients shared many char- acteristics of patients typically treated in hospital-based emergency departments. The outcomes of this population are also similar to those of an ED- based population with 5.8% with NSTEMI, 3.2% requiring urgent PCI, and 1.3% with STEMI.
The implication of our findings to the US healthcare system is worthy of consideration. The UCCs included in this study evaluated 48,958 patients (35,577 adult patients) during the study period. The Urgent Care Association estimates there are 130.6 mil- lion patient visits to urgent care centers each year.15 Based on our data indicating 1% of study patients present with chest pain or other symptoms concerning for ACS, we would speculate that over 1.3 million patient visits to urgent care centers annually are for these same symptoms.
Appropriate medical care was enhanced in our population by the incorporation of UCCs into our regional ACS network. UCC-specific protocols were developed and implemented that included a point-of-care troponin assay and pharmacologic therapy tailored to drugs easily stocked at UCCs. Prompt activation of the EMS system occurred via protocol guidelines that allowed for additional therapies, such as IV heparin and clopidogrel, to be administered by emergency medical personnel. Thus, this approach to treatment of UCC patients with possible ACS combined aspects of care typically rendered in non-medical facilities with treatments typically provided in EDs.
In the coming years, UCCs will play an increasing role in ambulatory care. It is estimated that the number of UCCs will continue to increase, with demand driven by patients looking for alternatives to overcrowded EDs with long wait times. While UCCs are designed to manage low-acuity patients, our study suggests that patients presenting with ACS are also encountered and should receive rapid and optimal care. Therefore, UCCs need to be incorporated into the planning and operation of pre-hospital systems of cardiac care with specific protocols for triage and integration of emergency medical transport in an effort to optimize the outcomes for this important and under recognized population of patients.
Despite its limitations, this study reflects the importance of identifying safe and effective mechanisms for outpatient evaluation and triage of patients with possible ACS. Additional study is necessary to determine the reproducibility of our data with greater statistical power. Recent studies have examined the use of “high-sensitivity” point-of-care troponin assays and their utility as a single measurement triage assay for possible ACS. While the use of these high-sensitivity assays may result in high false-positive rates, the potential for these tests as a triage tool in the outpatient setting is worth examining. Currently there exists no effective or accurate way to triage patients with possible ACS in the outpatient setting despite the large number of patients who present with these symptoms. Low specificity and high sensitivity in this population may be acceptable given the poor sensitivity and specificity of current mechanisms for evaluating these patients in the outpatient setting.
References
- Anderson JL, Adams CD, Antman EM, et ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50(7):e1-e157.
- Rathore SS, Epstein AJ, Nallamothu BK, Krumholz Regionalization of ST-segment elevation acute coronary syndromes care: putting a national policy in proper perspective.J Am Coll Cardiol. 2006;47(7):1346-1349.
- Jacobs AK, Antman EM, Ellrodt G, et Recommendation to develop strategies to increase the number of ST-segment-elevation myocardial infarction patients with timely access to primary percutaneous coro- nary intervention. Circulation. 2006;113(17):2152-2163.
- Rokos IC, French WJ, Koenig WJ, et Integration of pre-hospital electrocardiograms and ST-elevation myocardial infarction receiving center (SRC) networks: impact on Door-to-Balloon times across 10 independ- ent regions. J Am Coll Cardiol. 2009;2(4):339-346.
- Diercks DB, Kontos MC, Chen AY, et Utilization and impact of pre-hospital electrocardiograms for patients with acute ST-segment elevation myocardial infarction: data from the NCDR (National Cardiovascular Data Registry) ACTION (Acute Coronary Treatment and Intervention Outcomes Network) Registry. J Am Coll Car- diol. 2009;53(2):161-166.
- Pedersen SH, Galatius S, Hansen PR, et Field triage reduces treatment delay and improves long-term clinical outcome in patients with acute ST-segment elevation myocardial infarction treated with primary per- cutaneous coronary intervention. J Am Coll Cardiol. 2009;54(24):2296-2302.
- Ting HH, Krumholz HM, Bradley EH, et Implementation and integration of prehospital ECGs into systems of care for acute coronary syndrome: a scientific statement from the American Heart Association Inter- disciplinary Council on Quality of Care and Outcomes Research, Emergency Cardiovascular Care Commit- tee, Council on Cardiovascular Nursing, and Council on Clinical Cardiology. Circulation. 2008;118(10):1066-1079.
- Sivagangabalan G, Ong AT, Narayan A, et Effect of prehospital triage on revascularization times, left ventricular function, and survival in patients with ST-elevation myocardial infarction. Am J Cardiol. 2009;103(7):907-912.
- Rathore SS, Curtis JP, Chen J, et Association of door-to-balloon time and mortality in patients admit- ted to hospital with ST elevation myocardial infarction: national cohort study. BMJ. Clinical research ed. 2009;338:b1807.
- Urgent Care Association of http://www.ucaoa.org/home_abouturgent-care.php. Accessed April 15, 2010.
- Antman EM, Cohen M, Bernink PJLM, et The TIMI Risk Score for Unstable Angina/Non-ST Elevation MI: A Method for Prognostication and Therapeutic Decision Making. JAMA. 2000;284(7):835-842.
- Nawar EW NR, Xu National Hospital Ambulatory Medical Care Survey: 2005 Emergency Department Summary 2007. http://www.cdc.gov/nchs/data/ad/ad386.pdf
- Wright RS, Kopecky SL, Timm M, et Impact of community-based education on health care evaluation in patients with acute chest pain syndromes: the Wabasha Heart Attack Team (WHAT) project. Fam Pract. 2001;18(5):537-539.
- Dracup K, McKinley S, Riegel B, et A randomized clinical trial to reduce patient prehospital delay to treatment in acute coronary syndrome. Circ Cardiovasc Qual Outcomes. 2009;2(6):524-532.
- Weinick RM, DesRoches CM, Bristol Urgent Care Benchmarking Study Results. Warrenville, IL: Urgent Care Association; 2008.
