Published on
Urgent message: For patients with flu-like symptoms, a careful history and examination are important to rule out more threatening diagnoses.
SHRINESH V. PATEL, MD
Overview
In late winter/early spring, urgent care providers often encounter patients with flu or flu-like illnesses. It is easy to assume that an individual with a typical pattern of flu-like symptoms has the flu and not consider other pathologic processes.However, alternative diagnoses should always be in the differential, and careful history, examination, and testing can provide the clues necessary to identify more threatening diagnoses. Patients often present with attempts at self-diagnosis, but a clinician should be sure to gather a more open-ended history of present illness that focuses on signs and symptoms rather than accepting a patient’s interpretation.
Case Presentation
A 43-year-old African-American male presents with a history of “the flu” for the past 6 days. Over the past 2 days, he reports feeling worse, with complaints of increased body aches. The patient denies current sore throat, stuffy nose, or cough, but reports chills, sweats, and headache.
The man has generalized abdominal pain but denies burning on urination, urinary urgency or frequency, or penile discharge, and he has no nausea, vomiting, or diarrhea. However, he has noticed some blood in his urine. Socially, the patient drinks 2 to 3 beers on the weekend but denies illicit drug abuse and is a non- smoker. On initial presentation of the man, nothing abnormal is observed and he is alerted and oriented to person, place, and time. When questioned, he is cooperative and talks in complete sentences, while periodically playing with a video game on his phone
Observation and Findings
Physical examination of the patient reveals the following: Height: 6 feet
Weight: 160 kg Temp: 98.6°F RR: 15
BP: 130/70; P: 67 SpO2: 97% on RA
HEENT: PERRL EOMI, anicteric sclerae, pink oral
mucosa, no lesions, no LAD, TM normal bilaterall
Chest: CTA b/l no wheezing or rales
Heart: RRR no murmurs
Abd: Soft, n/d, mild TTP around umbilicus, no supra- pubic tenderness, +bs
Ext: No edema +2 pulses
Neuro: CN II-XII intact, light touch sensation intact, negative Romberg, no asterixis
As the patient is walking to the bathroom to gather a urine sample, he is noted to drag his right leg. He also has tenderness to palpation in his mid back, forearms, and especially in his right upper thigh.
Labs/Imaging
Urinalysis reveals slightly tea-colored urine and the fol- lowing:
Bld: 250 Ery/microliter +++ Protein: 5 g/L +++
Nitrite: Neg Ket: Neg Glu: Neg pH: 5.0
SpG: 1.025
Leu: 25 leukocytes/microliter +
Differential Diagnosis
Initially, this patient was thought to have a flu-like viral syndrome or a urinary tract infection, given his initial presentation. However, the significant musculoskeletal tenderness in his right quadriceps muscle and the dramatic limp observed led to a concern about rhabdomyolysis as the cause of the man’s symptoms. This preliminary conclusion was reinforced by the profound proteinuria and hematuria reported on urinalysis. Venipuncture for complete metabolic panel was attempted, but it was unsuccessful.
Hospital Course
Although detailed records of the patient’s hospital course were not obtained, follow-up with him confirmed the diagnosis of rhabdomyolysis. The patient’s creatine kinase was over 100,000. Vigorous hydration over the course of 4 days resulted in normalization of his renal function and CK. Infection was ruled out and no antibiotics were subsequently administered. The final cause of his rhabdomyolysis was not determined.
Discussion
Rhabdomyolysis is as an acute, fulminating, potentially fatal disease of skeletal muscle that entails destruction of muscle as evidenced by myoglobinemia and myoglobinuria.1 Many cases of rhabdomyolysis are associated with crush injuries, overexertion such as in marathon runners, use of medications such as corticosteroids, and exposure to toxic substances such as alcohol and cocaine. Inflammatory muscle disease such as polymyositis predisposes a patient to rhabdomyosis. In rare cases, a muscular genetic disorder can lead to the syndrome.
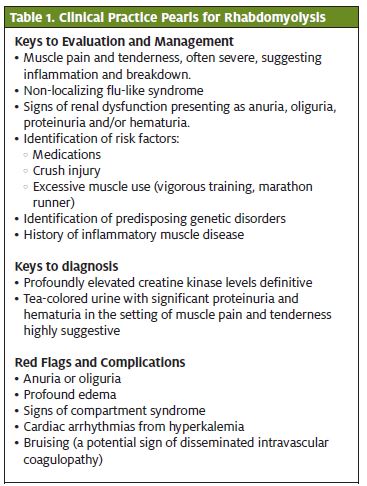
An infectious prodrome, including common viral and bacterial illnesses, is common in patients with rhabdomyolysis and it can lead to delayed diagnosis due to overlapping symptomatology. Clinical features include fatigue, severe muscle aches, and tea-colored urine. Screening tests include urinalysis with positive dipstick for blood, and creatine kinase levels (Table 1).2 According to 2005 non-federal hospitals discharge data, 23,000 cases of rhabdomyolysis were documented out of roughly 34.7 million hospital discharges.3 Even though the incidence is low, rhabdomyolysis has pro- found consequences for patients. It is only a matter of
time before their myoglobinuria leads to intrinsic renal failure. With such acute renal failure, ensuing metabolic and electrolyte derangements can lead to lactic acidosis, arrhythmias, and eventually mortality.
The mainstay of treatment for rhabdomyolysis is vigorous hydration to preserve renal function and correct any electrolyte imbalance. The rapid muscle breakdown leads to massive fluid loss and sequestration in dead muscle tissue. Therefore, fluid resuscitation should be initiated as quickly as possible. Acute renal failure can usually be reversed with hydration alone, but the myoglobin itself can cause a toxic tubular necrosis that can result in chronic renal failure despite hemodialysis. Pre-existing renal dysfunction increases this risk.
Conclusion
This patient presented to the urgent care clinic complaining of a typical flu-like illness, but strikingly had worsening body aches some blood in his urine 6 days after its onset. Urinalysis confirmed significant proteinuria and examination was notable for considerable musculoskeletal tenderness, all of which raised concern for muscle injury and breakdown. In this case, risk factors for rhabdomyolysis were not obvious but the diagnosis was suspected and later confirmed. With vigorous hydration, his CK normalized and his renal function was preserved. ■
References
- Stedman’s Concise Medical Dictionary for the Health 4th ed. Philadelphia: Lippincott Williams & Wilkins, 2001.
- Sauret JM, Marinides G, Wang Rhabdomyolysis. Am Fam Physician., 2002;65(5):907- 913.
- DeFrances CJ, Cullen KA, Kozak National Hospital Discharge Survey: 2005 annual summary with detailed diagnosis and procedure data. National Center for Health Statistics. Vital Health Stat 13(165). 2007.