Published on
Urgent Message: The diagnosis of bacterial pharyngitis is often difficult. Rapid polymerase chain reaction testing has potential to improve diagnostic certainty. Despite high accuracy rates, many urgent care providers continue to seek confirmation by throat culture.
Justin Bowles, MD, Supreet Ghumman, MS4
Citation: Bowles J, Ghumman S. Real world validation of rapid PCR strep testing in urgent care. J Urgent Care Med. 2023;18(2):15-21
Key Words: bacterial pharyngitis; PCR testing
Abstract
Introduction: Point-of-care polymerase chain reaction (PCR) testing for strep pharyngitis has recently been adopted as the preferred method of rapid testing for pharyngeal group A strep (GAS) infection in many urgent care (UC) centers. Despite the high published accuracy of PCR for GAS (sensitivity 94.2% and specificity 98%), many medical providers continue ordering confirmatory throat cultures.
Methods: This was a multisite retrospective chart review of patients seen throughout a regional network of UC centers in Washington state who were tested for GAS. Patients were included if they had a resulted strep PCR and throat culture to validate the accuracy of the point-of-care testing (POCT) strep PCR in a real-world setting.
Results: A false negative PCR result (PCR -, culture +) was identified in only 6 cases (2.3%). True negative PCR findings (PCR -, culture -) resulted in 247 cases (95.7%). Specificity was calculated to be 99.3% (NPV= 97.6%), which closely approximates the manufacturer’s reported value. Five patients were identified as having a true positive test (PCR +, culture +), and two had a false positive (PCR +, culture -). Non-GAS, not testable with this PCR strep test machine, was revealed on 7% (26/383) of all throat cultures. An antibiotic was prescribed presumptively in 42% (159/383) of cases. Oral steroids were given for symptomatic treatment in 129 of the 383 (33.6%) cases. Centor scores were calculated for all patients. No difference in the average scores was identified when calculated for the several subcategories of patients identified to have GAS, non-GAS, true positive, true negative, false positive, or a false negative. Each category scored approximately 2 out of 5 (range: 1.8–2.2), suggesting that throat cultures were being used for confirmation on the least obvious cases.
Conclusion: Despite excellent specificity, ordering of confirmatory throat cultures was common in this urgent care network. This practice as well as presumptive antibiotic treatment while culture is pending suggests a lack of clinician confidence in the validity of a negative PCR strep test result. The test characteristics in this chart review study correspond with the industry published specificity of POCT strep PCR testing and should reassure acute care providers as they incorporate this new technology into their practice.
Introduction
Acute pharyngitis is among the most common conditions encountered in outpatient clinical practice in the United States.1,2 Although most cases of acute pharyngitis are caused by respiratory viruses, group A streptococcus (GAS), also known as Streptococcus Pyogenes, is responsible for 5%–15% of cases in adults and 20%–30% of cases in children. It is the most common bacterial pathogen involved in cases of pharyngitis in children and adolescents.3,4
Clinical diagnosis of GAS pharyngitis is challenging due to its overlapping symptomatology with other infectious and non-infectious etiologies.5,6 The Centor Score has been an essential part of acute pharyngitis assessment for over 30 years in adults.7 The original Centor criteria were later modified by McIsaac et al. in 1998 to include age. This addition allowed its use for children.8
A score of 4 or greater correlates with a 56% probability of a GAS-positive culture. This clinical assessment tool helps differentiate GAS from other etiologies of pharyngitis, however, it is not sensitive or specific enough to definitively rule in or rule out GAS infection.7,8 Rapid antigen detection tests (RADT) for GAS are common in the acute care setting, however their sensitivities are generally <90%,9 and therefore the Infectious Disease Society of America (IDSA) recommends that negative RADT be confirmed via throat culture for all children.5
Point-of-care laboratory testing (POCT) involving polymerase chain reaction (PCR) technology is a recent addition to many urgent care clinics. PCR strep testing has been shown to be more accurate than antigen testing and significantly decreases inappropriate antibiotic use.10 Nascent bedside PCR tests, like those for COVID-19 and influenza, lack an immediately available gold standard for comparison, requiring clinicians to rely on industry-published accuracy data.
Study Design
The Cobas Liat® strep A nucleic acid test became available in the urgent care clinics involved in this study in Washington state in 2022. Despite the industry-published sensitivity and specificity of 94.2% and 98% respectively,11 many clinicians continued to seek confirmation rapid PCR tests by throat culture. This practice style created an opportunity to validate the accuracy of the POCT strep PCR machine under real-world conditions.
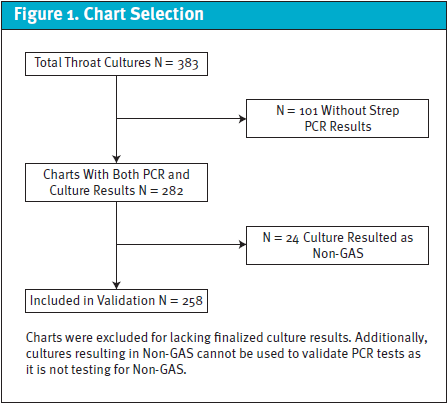
All visits with either a rapid strep test or throat culture ordered during the 3-month period of August 2022 to October 2022 by 71 medical providers at 32 different Indigo Urgent Care centers in Washington state were screened for eligibility. From there, 418 charts were identified. Thirty-five of these cases lacked a finalized throat culture (Figure 1). A recent PCR strep test (within the previous 7 days) was not available in 101 cases, yielding 282 patient encounters with both a resulted PCR test and a corresponding throat culture. Twenty-four patients had group C strep or group G strep (non-GAS) growth on the throat culture.
The Cobas Liat ® strep A nucleic acid test was used for PCR testing; it does not detect non-GAS strains. Therefore, these charts were also excluded from the PCR test validation, although they are included in calculations not involving PCR results. The PCR test findings were compared with the culture result as a gold standard to categorize each as a true or false, positive or negative PCR result in the remaining 258 charts. The project was reviewed by the MultiCare Institutional Review Board and given a waiver given its retrospective design as a chart review study.
Results
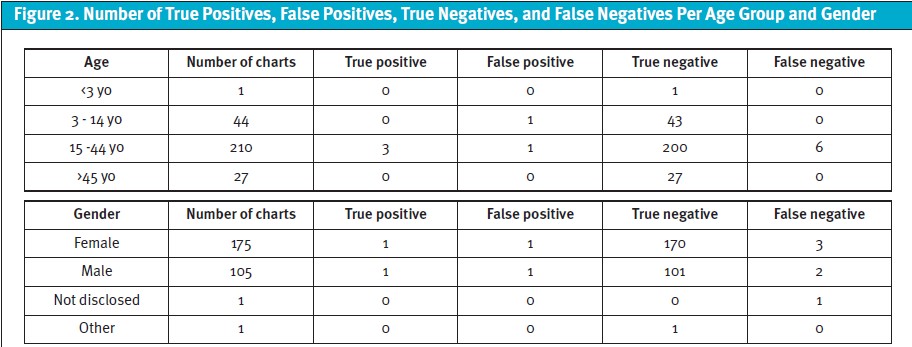
Demographic information was collected on the 282 charts with both rapid PCR and strep culture results. Despite the higher incidence of strep throat among pediatric patients, only 44 of the 282 (16%) charts reviewed were younger than 14 years old. All 6 of the cases with a negative PCR and a positive throat culture (the false negatives) were in the category of 15 to 44 years old. Sixty-two percent of the study participants were female (175/282). The incidence of a false negative PCR result was very similar between males and females at 2:3 (Figure 2).
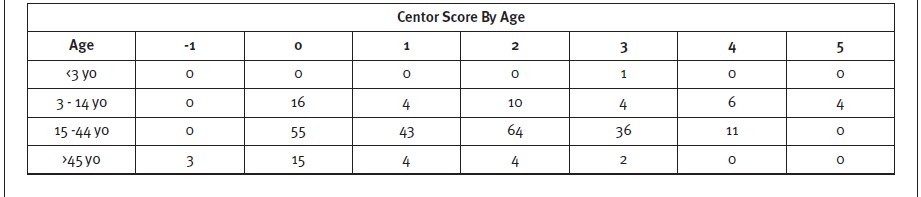
Centor scores were categorized according to age. The patients who scored the highest Centor value of 5 were all in the age group of 3 to 14 years old, and the lowest possible score of -1 was only found in those >45 years old. This is not surprising because in the age-modified Centor scoring, a point is added for patients 3 to 14 years old, and a point is subtracted for patients >45 years old.
The throat culture was positive in 9 of the cases included for validation. Three of these culture positive cases had a previous positive PCR, representing a true positive PCR result (1.2%, 3/258). The 6 remaining positive throat cultures had a corresponding negative PCR. This signifies a false negative PCR rate of 2.3% (6/258). Some 247 charts revealed both a negative PCR and negative throat culture, resulting in a true negative rate of 95.7%. Two cases were identified as having a positive PCR test that later yielded a negative culture, denoting a false positive result (0.8%, 2/258), given that the throat culture is the gold standard of comparison. Subsequently, the specificity was calculated to be 99.2% (NPV= 97.6%). From the available data included in this study, the sensitivity was 30% (PPV 60%). Non-GAS was identified on 7% (26/383) of the throat cultures (Figure 3).

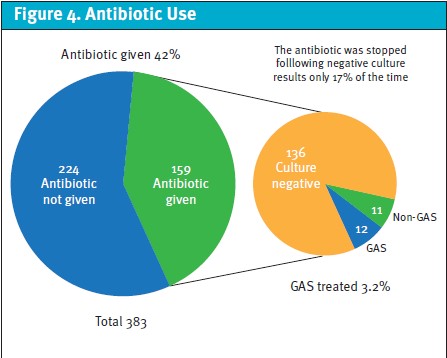
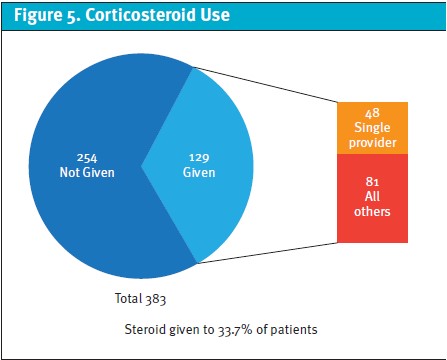
A total of 383 charts included a throat culture result allowing a strep infection to be confidently identified. An antibiotic was empirically prescribed in 42% (159/383) of cases (Figure 4). The culture was negative in 136 charts. Thus, a bacterial infection was present in 6.0% (23/383) of individuals. Only 11 of these infections were confirmed to be due to GAS. Of the 383 patient charts reviewed, steroids were prescribed in 129 cases (33.7%).
The rate of empiric antibiotic therapy and symptomatic steroid treatment is highly variable between medical providers. It was observed that a single provider, who participated in 14% of the patient encounters (59/418), ordered 37% (48/129) of the total number of corticosteroids and 26% (41/159) of the total antibiotic prescriptions. When this provider’s data is excluded as an outlier, the rate of antibiotics and corticosteroids prescribed decreases by 6% (118/324, 36%) and 8% (81/324, 25%), respectively.
Discussion
This study provides real world validation for the Cobas Liat® strep A nucleic acid test by revealing a specificity (99.2%) very near the published value of 98%. Due to a relatively low number of PCR positive results having an associated throat culture (N=5), the calculated sensitivity of 30% is almost certainly spurious and related to the appropriate practice of not sending cultures when initial POCT PCR testing is positive.
The throat culture revealed non-GAS as a possible cause of the patient’s pharyngitis in 26 cases. Rapid PCR testing for S. pyogenes does not evaluate for non-GAS strains, thus corresponding PCR tests are expected to be negative. The primary goal for antimicrobial therapy of bacterial pharyngitis, according to the IDSA, is for the prevention of acute rheumatic fever and suppurative complications including peritonsillar abscess, cervical lymphadenitis, and mastoiditis.6 Non-GAS pharyngitis is not known to trigger acute rheumatic fever. Also, patients with group C and G strep frequently experience less severe symptoms of fever, throat erythema, and lymphadenopathy and higher rates of cough and rhinorrhea when compared with those with group A strep; therefore, treatment of non-GAS is felt to be of little benefit. When treatment is indicated, the same regimens recommended for GAS pharyngitis are suitable for non-GAS, yet a course of 5 days (rather than 10 days) is reasonable.12 For these reasons, these 26 charts were not included in the overall analysis.
Patients with pharyngitis are frequently treated empirically with antibiotics pending throat culture results. In this study population, an antibiotic was prescribed in 42% of cases (Figure 4). A bacterial infection, however, was present in only 6.0% of individuals. As treatment of non-GAS is often not appropriate, antibiotics were likely only indicated in 2.9% of the cases. This high rate of presumptive treatment suggests a lack of confidence in the accuracy of a negative PCR test and a general trend to overprescribe antibiotics for pharyngitis in UC.
This is significant because, according to the IDSA clinical practice guidelines, “with the exception of very rare infections by certain other bacterial pharyngeal pathogens (eg, Corynebacterium diphtheriae and Neisseria gonorrhoeae), antimicrobial therapy is of no proven benefit as treatment for acute pharyngitis due to organisms other than GAS.”5 Best practice for appropriate antibiotic stewardship, in the case that a patient is treated presumptively for GAS, would be to discontinue treatment as soon as the culture resulted negative. This occurred only 17% of the time (23/136).
Despite only mild benefit, the availability of other analgesics with significantly fewer risks, and the IDSA guidelines recommending against the use of glucocorticoids, oral steroids were prescribed in over one-third (33.7%) of cases by the providers in this study for symptomatic treatment of sore throat (Figure 5).5, 13 While corticosteroids have been shown to decrease the duration and severity of symptoms in GAS pharyngitis, the actual reduction in pain duration is less than 6 hours on average.13
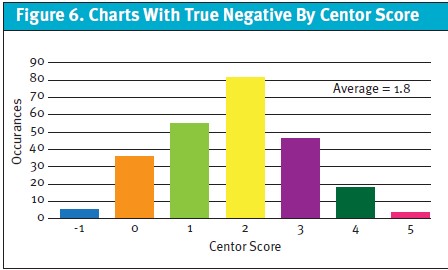
Centor scores were calculated for all patients with a strep PCR and throat culture result to objectify severity and hint which patient presentations prompt the ordering of a throat culture to confirm a PCR test. The Centor Criteria is a scale from -1 to 5, assigning points for age, fever, lack of cough, tender or swollen anterior cervical lymph nodes, and tonsillar swelling or exudate. No substantial difference was identified in the average Centor score for any of the studied subgroups; culture identified GAS (2.1) and non-GAS (1.8), or true positive (2.0), false positive (2.0), false negative (2.2), and true negative (1.8) PCR results (Figure 6).
Finally, several charts were excluded from the study because the throat culture was part of a sexually transmitted disease work up. This hints that some medical providers do not understand which organisms grow on this throat culture medium or what specific tests are appropriate when a patient being evaluated for a sexually transmitted disease also has complaints of a sore throat.
Limitations
This chart review study includes important and noteworthy limitations. Most importantly, the study was retrospective in design and involves only chart review. It is unclear why certain providers may or may not have ordered confirmatory cultures in cases of negative rapid PCR testing. Moreover, it is unlikely that the 71 medical providers included in the study were operating under a single rationale when deciding to order a throat culture or treat with an antibiotic or steroid. It cannot even be assumed that a single provider used similar logic with each patient they evaluated. There are many reasons that one may opt for these tests and treatments. This may include patient request or concern, provider practice habits, previous poor outcome, practicing defensive medicine, conservative practice style, or even electronic medical record order sets.
The study was conducted over only a 3-month period in the late summer and fall. It is unclear whether test ordering and prescribing patterns may have had seasonal variability based on this limited period of data collection.
Another limitation to this study is that strep PCR tests and throat cultures in the UC clinics require different swab material and collection medium, thus some of the variability between PCR and throat culture practices may result from swab collection quality. In real-world conditions, the quality of the sample collected cannot be standardized and will vary between providers.
Conclusion
As new point-of-care testing becomes available for use, providers are confronted with the dilemma of whether and how to change their practice. In the summer of 2022, our network of UC clinics was confronted with this situation when PCR GAS testing became available for use, touting a highly accurate result in 20 minutes. In many cases, medical providers in our centers continued to order confirmatory throat cultures despite usually negative results.
False negative PCR tests were rarely identified by throat culture with a specificity of 99.3% (NPV= 97.6%). These results correspond with the industry reported values and offer reassurance to acute care practitioners that this technology is safe to include in their practice.
Non-GAS was discovered on 7% of all throat cultures included in the study. Non-GAS pharyngitis symptomatology is frequently less severe, suppurative complications are fewer, and do not lead to rheumatic fever when comparted to GAS.14,15 Thus, the significance of identification and treatment are controversial. As non-GAS species are not tested on with the PCR test, culturing the throat to identify group C strep or group G strep is not a valid clinical rationale for obtaining a culture.
In the charts reviewed, antibiotics were prescribed 13 times more often than indicated. This surprisingly high rate of antibiotic treatment suggests that UC providers may overestimate the incidence of GAS, or patient satisfaction may be trumping antibiotic stewardship.16 Additionally, oral steroids, which are rarely indicated, were used for symptomatic treatment in over one-third of the patient encounters.
Our data also suggest that the rate of empiric antibiotic therapy and symptomatic steroid treatment is highly dependent on practice styles. For example, a single provider who participated in 60 of the 415 patient encounters (14%) ordered 38% (49/129) of the total number of corticosteroids and 25% (41/161) of the antibiotics.
This study was designed to validate the rapid strep PCR test to determine the necessity of confirmatory throat cultures following a negative result. A future quality improvement study could include presenting our internal data to medical providers and conducting a post-intervention chart review to evaluate if any change in practice was achieved. Additionally, a more accurate sensitivity could be assessed by requesting that medical providers order throat cultures after a positive PCR for a short, specified period of time. However, the ethics of this study would be problematic unless there were funding to ensure the cost of these mostly unnecessary cultures is not passed on to the patients.
The accurate diagnosis of GAS pharyngitis has been a perpetual and central issue for acute care clinics. Clinical criteria in combination with POCT can aid this evaluation. The advent of rapid PCR testing has the potential to improve diagnostic accuracy and decrease the inappropriate use of antibiotics. Confirmatory throat cultures and presumptive antibiotic treatment increases cost and risk to the patient. This chart review supports the industry published specificity of POCT GAS PCR testing and should offer reassurance for UC clinicians as new technology is increasingly integrated into UC practice.
REFERENCES
- Centers for Disease Control and Prevention. Erythromycin-Resistant Group A Streptococcus. Centers for Disease Control and Prevention; 2019. Accessed August 30, 2023. https://www.cdc.gov/drugresistance/pdf/threats-report/gas-508.pdf
- Ebell, M. H., Smith, M. A., Barry, H. C., Ives, K., & Carey, M. (2000). The rational clinical examination. Does this patient have strep throat? JAMA, 284(22), 2912–2918. https://doi.org/10.1001/jama.284.22.2912
- Kronman, M. P., Zhou, C., & Mangione-Smith, R. (2014). Bacterial prevalence and antimicrobial prescribing trends for acute respiratory tract infections. Pediatrics, 134(4), e956–e965. https://doi.org/10.1542/peds.2014-0605
- Bisno A. L. (1996). Acute pharyngitis: etiology and diagnosis. Pediatrics, 97(6 Pt 2), 949–954.
- Bisno, A. L., Gerber, M. A., Gwaltney, J. M., Jr, Kaplan, E. L., & Schwartz, R. H. (1997). Diagnosis and management of group A streptococcal pharyngitis: a practice guideline. Infectious Diseases Society of America. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America, 25(3), 574–583. https://doi.org/10.1086/513768
- Wannamaker L. W. (1972). Perplexity and precision in the diagnosis of streptococcal pharyngitis. American Journal of Diseases of Children (1960), 124(3), 352–358. https://doi.org/10.1001/archpedi.1972.02110150050009
- Centor, R. M., Witherspoon, J. M., Dalton, H. P., Brody, C. E., & Link, K. (1981). The diagnosis of strep throat in adults in the emergency room. Medical Decision Making: an International Journal of the Society for Medical Decision Making, 1(3), 239–246. https://doi.org/10.1177/0272989X8100100304
- McIsaac, W. J., White, D., Tannenbaum, D., & Low, D. E. (1998). A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ: Canadian Medical Association Journal (Journal de l’Association Medicale Canadienne), 158(1), 75–83.
- Cohen, J. F., Bertille, N., Cohen, R., & Chalumeau, M. (2016). Rapid antigen detection test for group A streptococcus in children with pharyngitis. The Cochrane database of systematic reviews, 7(7), CD010502. https://doi.org/10.1002/14651858.CD010502.pub2
- Rao A., Berg B., Quezada T., et al. Diagnosis and antibiotic treatment of group a streptococcal pharyngitis in children in a primary care setting: impact of point-of-care polymerase chain reaction. BMC Pediatrics. 2019 Jan;19(1):24. DOI: 10.1186/s12887-019-1393-y. PMID: 30651115; PMCID: PMC6335697.
- Roche Diagnostics. Accessed August 30, 2023. https://diagnostics.roche.com/us/en/products/instruments/cobas-liat-ins-6050.html
- Kakuya, Fujio et al. “Acute Pharyngitis Associated with Streptococcus dysgalactiae Subspecies equisimilis in Children.” The Pediatric Infectious Disease Journal. 37 (2017): 537–542.
- Olympia, R. P., Khine, H., & Avner, J. R. (2005). Effectiveness of oral dexamethasone in the treatment of moderate to severe pharyngitis in children. Archives of Pediatrics and Adolescent Medicine. 159(3), 278-282. https://doi.org/10.1001/archpedi.159.3.278
- Denny, F. W., Wannamaker, L. W., Brink, W. R., Rammelkamp, C. H., Jr, Custer, E. A. (1950). Prevention of rheumatic fever; treatment of the preceding streptococcic infection. Journal of the American Medical Association. 143(2), 151–153. https://doi.org/10.1001/jama.1950.02910370001001
- Frost, H. M., Fritsche, T. R., & Hall, M. C. (2019). Beta-Hemolytic Nongroup A Streptococcal Pharyngitis in Children. The Journal of Pediatrics. 206, 268–273.e1. https://doi.org/10.1016/j.jpeds.2018.10.048
- Poses, R. M., Cebul, R. D., Collins, M., & Fager, S. S. (1985). The accuracy of experienced physicians’ probability estimates for patients with sore throats. Implications for decision making. JAMA, 254(7), 925–929.
Author Affiliations: Justin Bowles, MD, MultiCare Health System, Tacoma, Washington. Supreet Ghumman, MS4, Pacific Northwest University of Health Sciences, Yakima, Washington.