Published on
Urgent message: Abdominal pain can be a challenging complaint, especially in younger patients. Consider the full range of differential diagnosis in order to initiate prompt, effective management.
Curtis Kommer MD, Latha Shankar, MD, MBA and Robert Stuart, MD
Introduction
Since the time of Hippocrates, the ability of physicians to unravel the mystery of a patient’s abdominal pain has become synonymous with the art and practice of medicine. Pediatric abdominal pain, in particular, with its extensive differential diagnosis and limitations in history-taking and physical exam, can be a challenging presentation to an urgent care provider.
The following case presentation of a 6-year-old boy with abdominal pain offers insight – and, we hope, some useful navigational tools – into the importance of a sound knowledge of the differential diagnosis.
Case Presentation
I.R., a 6-year-old boy, was brought to the Aurora Urgent Care Center by his mother. She related a three-day history of abdominal pain, lack of appetite, and occasional vomiting. No fever had been appreciated, and they had not noticed diarrhea or bloody emesis. An infrequent, dry cough was mentioned, but no other coryzal symptoms.
There was no history of recent trauma, any recent travel or exposures, and the child’s past medical and surgical history was negative.
I.R. appeared mildly ill and fatigued, with dry mucus membranes. In addition, we found:
- temp: 100.2
- pulse: 126
- respirations: 24/min
- % O2 sat 99%
Skin and EENT exam were normal.
Auscultation of the chest revealed left basilar rales.
Abdominal exam showed a scaphoid, soft abdomen with no organomegaly or mass, active bowel sounds, and mild tenderness to palpation in the left upper quadrant.
Rectal exam was deferred. Genitalia was normal.
Focus on the Potential Causes
Although the causes of pediatric abdominal pain can vary by age (Table 1), various studies have shown the most common, overall identifiable diagnosis is constipation (48%), followed by gastroenteritis (28%).
Surgical causes were identified in < 2% of pediatric abdominal pain presentations.
The most common extra-abdominal causes include pneumonia (up to 5% of abdominal pain visits), pharyngitis, and acute leukemia.
Reviewing the differential diagnosis for each child presenting with abdominal pain can serve as a critical reminder to:
- identify life-threatening or surgical problems (e.g., appendicitis, torsion, ectopic pregnancy)
- consider atypical diagnoses needing treatment (e.g., abuse, diabetes, infection)
- perform a through exam, including the chest, groin, and recto-vaginal areas, as necessary
- order timely and appropriate studies, as needed.
A basic mnemonic device for pediatric abdominal pain (such as seen in Table 2) can be a helpful tool for the busy clinician; an example of using the history and physical findings to narrow the diagnostic considerations is presented in Figure 1.
Table 1. Potential Causes of Stomach Pain in a Child |
|||
| Syndrome | Typical cause | Age group | Typical clinical syndromes |
| Bacterial | Pneumococcus; others | All ages (< 6 y more common) | · Abrupt onset · High fever · Ill/toxic appearance, more focal findings on examination · Chest/abdominal pain, focal infiltrate if CXR is obtained |
| Atypical – infancy | Chlamydia trachomatis | < 3 mo | · Tachypnea · Mild hypoxemia · Lack of fever · Wheezing · Interstitial infiltrates on chest x-ray |
| Atypical – older children | Mycoplasma | > 5 y | · Gradual onset · Low-grade fever · Diffuse exam findings – wheezes, diffuse infiltrates on chest x-ray |
| Viral | Multiple viruses | All ages (3 mo to 5 y more common) | · Prominent upper respiratory symptoms · Low-grade or absent fever · Diffuse exam findings on exam – wheezes possible, diffuse infiltrates on chest x-rays |
Table 2. “Abdominal Pain” Spells It Out |
|
| A | Appendicitis |
| B | Blood disorders (sickle cell, HSP, HUS, leukemia) |
| D | Diabetes (DKA) |
| O | Ovarian or testicular torsion |
| M | Malrotation (volvulus, intussusception, hernia) |
| I | Infection (pharyngitis, pneumonia, gastroenteritis) |
| N | Nephric (UTI, calculi, renal trauma) |
| A | Abuse |
| L | Lymphadenitis, mesenteric |
| P | Pregnancy/PID |
| A | Acid-peptic (PUD) |
| I | Inflammatory bowel disease |
| N | No stools (constipation) |
Pneumonia as a Cause of Abdominal Pain
As the most common extra-abdominal cause of childhood abdominal pain, pneumonia can also be a devastating diagnosis to miss, with significant morbidity and mortality.
Typically, children will present with cough, coryza, or other respiratory symptoms. Fever is the most reproducible sign, occurring in 83% of proven pneumonias.
The abdominal pain is the result of both visceral and somatic innervation of the diaphragm and peritoneum.
Irritation of these afferent pathways by a lower-lobe pneumonic infiltrate is usually experienced by the child as left or right upper quadrant abdominal pain, but can occasionally be referred to the lower abdomen, even mimicking appendicitis.
In the setting of abdominal pain, the presence of fever and respiratory symptoms may prompt the consideration of a chest radiograph, and possible admission, especially if any of the following are noted:
- Infant < 3-months-old
- Presence of other chronic medical conditions
- Oxygen saturation < 92%
- Respiratory rate > 70 (infant), >50 (older children), or respiratory distress
- Signs of dehydration
- Family unable to provide appropriate care or supervision
Case Follow-up
I.R.’s evaluation in the urgent care clinic included:
- normal HGB
- WBC elevated at 34,000
- sodium decreased at 129.
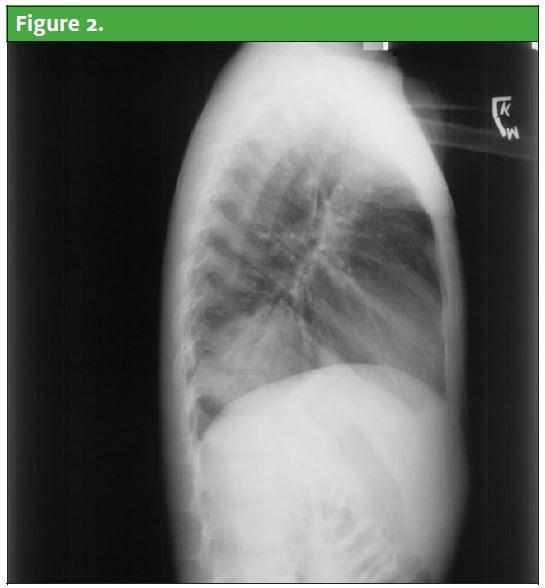
Chest radiograph revealed left lower lobe lung infiltrate (Figure 2 and Figure 3).
He was treated with oral acetaminophen, IV hydration, and a dose of IV ceftriaxone.
After a period of observation, he was felt to be clinically improved, afebrile, and comfortable, and was discharged with PO azithromycin and close primary care follow-up.

The Take-home Message
When faced with this chief complaint, reviewing the differential diagnosis for pediatric abdominal pain minimizes the potential for missing a serious diagnosis, and maximized the clinician’s ability to combine history, physical, and other findings to make the best possible diagnosis.
In this case, it allowed the urgent care clinician to consider an atypical, but will-known, cause of abdominal pain in children: pneumonia.
Keep this in mind when your next patient is a child with “belly pain.”
Resources
- Winsey HS, Jones PF. Acute abdominal pain in childhood: Analysis of a year’s admissions. BMJ. 1967; i: 653-655.
- WHO/UNICEF. Pneumonia – The forgotten killer of children. 2006; New York, NY.
- Stevenson RJ, Ziegler MM. Abdominal pain unrelated to trauma. Pediatr Rev. 1993; 14(8): 302-311.
- Leung AKC, Sigalet DL. Acute abdominal pain in children. AM Fam Physician. 2003; 67(11): 2321-2327.
- Durbin WJ, Stille C. Pneumonia. Pediatr Rev. 2008; 29(5): 147-160.

Curtis Kommer, MD
