Published on
Urgent message: As shown in an in-house study by one urgent care operator, protocol-driven, nurse-only care of specific presenting complaints may be one way to help curb healthcare spending while not compromising on quality of care or threatening patient-satisfaction scores.
Kyle Coon and Brett Whyte, MD
Abstract
Basic healthcare costs are rising at a staggering and, it’s widely considered, unsustainable rate. As a result, lower-cost alternatives that maintain quality and satisfaction are being explored across all care settings. One such initiative provides nurses at Winona Health Urgent Care with detailed algorithms to address common complaints such as sore throat and dysuria in otherwise healthy people for the purpose of comparing the overall quality, cost, and patient satisfaction of “nurse-only” care vs traditional provider care. The hypothesis that nurse-only care for these complaints maintains quality and patient satisfaction at a lower cost was tested through post-care telephone survey of patients. Patients must have met inclusion criteria for nurse-only care and be without exclusion criteria, in order to be considered for either arm of the study.1 Ten to 14 days post visit, qualified patients from either category were asked if they experienced an improvement or resolution of symptoms; if additional follow- up visit(s) were required for the same problem; and how they rank their overall satisfaction. Data were collected in aggregate form, leaving no patient identifiers, and analyzed for differences between provider and nurse-only categories. Lastly, cost of care for both groups was investigated in order to determine if the nurse-only protocol is a lower cost alternative to the traditional provider care. Collected data provided comparisons of satisfaction scores between both groups; tracked whether the need for additional visits for the same complaint was higher in the nurse-only category; and revealed the percentage of patients with resolution of symptoms between both groups. There was no statistical difference between the two groups in overall satisfaction, resolution of symptoms, or need for additional visits for the same problem. The nurse-only group had a much lower total cost of care to the patient.
Background
The total cost of care for basic healthcare services is staggering and widely considered unsustainable. Healthcare costs as a percent of gross domestic product (GDP) in the United States was 17.5% in 2014—higher than any other nation.2 In addition, healthcare consumer price index (CPI) has outpaced general CPI every year since 2008, indicating that the problem is worsening.3 Efforts to provide lower-cost alternatives to traditional care while maintaining quality and patient satisfaction are essential to meaningful reform. In the urgent care setting, isolated sore throats and uncomplicated dysuria are common chief complaints. We have developed “nurse-only” protocols for these chief complaints, encompassing the entirety of care. The Minnesota Board of Nursing was consulted to assure that the protocols were compliant with Minnesota statutes regarding condition specific protocols and fell within nursing scope of practice parameters. Previous studies have evaluated appropriate antibiotic prescribing habits retrospectively in patients with pharyngitis in nurse-only vs traditional care.4 Our goal was to evaluate this process prospectively for quality, cost, and satisfaction data and compare the nurse-only group with a group of patients with similar chief complaints seen by a physician or associate-level providers in the same clinic. To measure satisfaction and quality, data points for patient satisfaction with the process, resolution of symptoms, and frequency of repeat visits for the same complaint were collected. In addition, total cost of care was compared between the two groups.
Methods
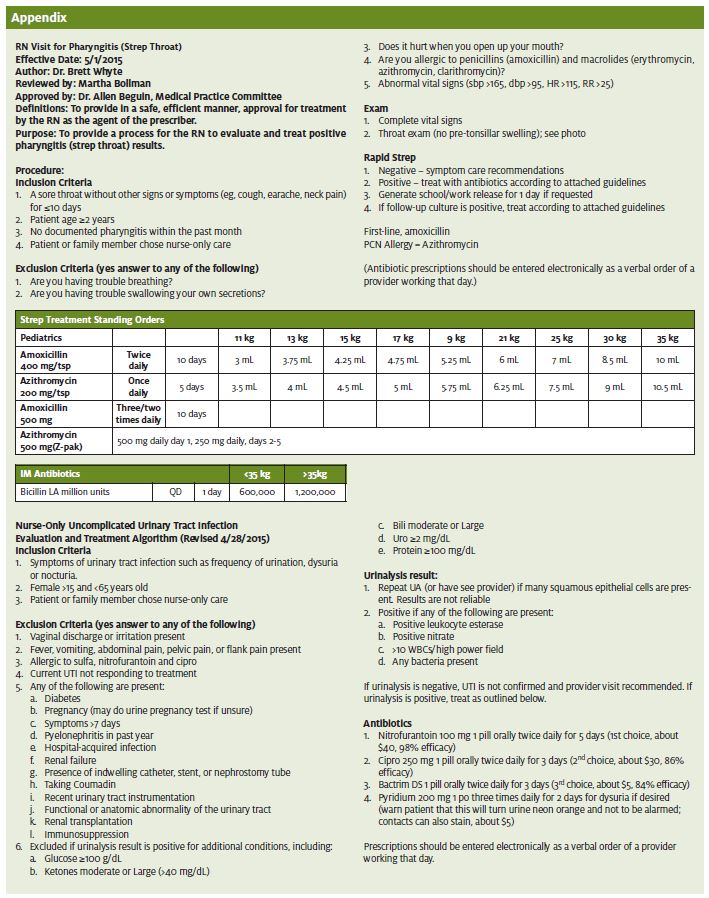
Patients seen in urgent care for isolated sore throats or dysuria and fulfilling inclusion criteria and not having any exclusion criteria (see Appendix) were included in the study.1 Patients who agreed to participate in the study were given the option of nurse-only protocol driven care vs traditional provider-based care, creating the two arms of the study. Patient interviews were conducted by the investigators for data collection by phone 10-14 days after the initial visit. If needed, a second or third phone call was made in this 4-day window before the patient was considered “lost to follow-up.” As part of the interview, patients were asked to rank their satisfaction with their visit on a scale from 0 (very unsatisfied) to 10 (very satisfied). Also, patients were asked if they required additional follow-up visits for the same complaint and to classify their clinical course of symptoms as either “worse,” “no change,” “improved,” or “resolved.” Patient questions during these phone calls were referred to appropriate licensed professionals when needed. Data were collected from January 2016 to March 2016. Statistical analysis of the data was performed, and comparisons were made between the nurse-only and traditional care groups using JMP Pro 12 statistical analysis software. There was no cost to subjects in excess of standard charges for similar patients not involved in the study.
Results
Data were recorded into categories, placing counts of 0-3 as unsatisfied, 4-6 as neutral, and 7-10 as satisfied.5 Table 1 was analyzed using Fisher’s Exact Test to determine if there was evidence that satisfaction scores were lower in the nurse-only group. It was found that Fisher’s Exact Test reported p-values >0.05 for categorical analyses (0.8378), denoting no evidence that the nurse-only group had lower satisfaction scores from patients than the provider group.
| Table 1. Data distribution among categorical satisfaction data for nurse-only and provider groups | ||||
| Unsatisfied (0-3) | Neutral (4-6) | Satisfied (7-10) | Total | |
| Nurse | 1 (0.40%) | 2 (0.81%) | 245 (98.8%) | 248 |
| Provider | 0 | 0 | 15 (100) | 15 |
| Total | 1 | 2 | 260 | 263 |
| P value: 0.8378 | ||||
The need for additional healthcare visits for the same problem was also examined between nurse-only and provider groups to measure quality. These data were collected by contacting patients over the phone and examined using JMP Pro 12 statistical analysis software. Data from Table 2 present no evidence that the need for additional healthcare visits is higher in the nurse-only group than in the provider group. This was determined using Fisher’s Exact Test to analyze the data in Table 2, which presented a p-value of 0.9459, (denoting no evidence of statistical difference between the two categories).
An additional aspect of this study tested if the percentage of patients with either improvement or resolution of symptoms 10-14 days after their visit was lower in the nurse-only group compared with the group that saw a provider. These data were also used as a variable to measure overall quality. Data for this examination were collected via patient survey over the phone. The patients were asked to categorize their clinical course into four groups: resolved, improved, no change, or worse. It was found that the nurse-only group did not present a lower rate of symptom alleviation than the provider group according to the p value obtained from Table 3’s data, 0.110.
| Table 2. Data distribution for additional healthcare visits among both nurse-only and provider groups | |||
| No | Yes | Total | |
| Nurse | 242 (97.6%) | 6 (2.4%) | 248 |
| Provider | 14 (93.3%) | 1 (6.7%) | 15 |
| Total | 256 | 7 | 263 |
| P value: 0.9459 | |||
| Table 3. Symptom resolution between nurse-only and provider groups | |||||
| Worse | No Change | Improved | Resolved | Total | |
| Nurse | 1 (0.4%) | 5 (2%) | 29 (11.7%) | 213 (85.9%) | 248 |
| Provider | 0 | 0 | 0 | 15 (100%) | 15 |
| Total | 1 | 5 | 29 | 228 | 263 |
| P value: 0.110 | |||||
Finally, a cost analysis was compared between nurse-only and provider groups.6 Cost for services of both complaints relating to tests for isolated sore throats (rapid strep test) and uncomplicated dysuria (urinalysis), as well as provider services charged by Winona Health Urgent Care, were examined. Both nurse-only and provider groups conduct a rapid strep screening for patients complaining of isolated sore throats to test for pharyngitis. Winona Health Urgent Care charges $86 for both groups for this service. Likewise, both groups conduct a urinalysis for patients complaining of dysuria to test for a urinary tract infection, which costs $33 for both groups. However, the provider group on average charges a fee of $151 for a level 3 office visit for both complaints, which presents the opportunity for cost savings for the nurse-only visit. The nurse-only group shows a total cost saving of 64% for visits regarding isolated sore throats and an 82% cost savings to patients for visits regarding dysuria compared with the provider group as seen in Table 4.
| Table 4. Service charges for each group and test performed for each complaint, as well as total cost for both types of complaints for each group, and the total cost reduction of the nurse-only group visit compared to the provider | |||
| Group/Service | Service/Charge | Average Total Cost per Service | Cost Analysis |
| Nurse-only –office charge | Level 3 office visit $0 | ||
| Isolated sore throat | Rapid strep test $86 | $86 | 64% cost reduction |
| Dysuria | Urinalysis $33 | $33 | 82% cost reduction |
| Provider – office charge | Level 3 office visit $151 | ||
| Isolated sore throat | Rapid strep test $86 | $237 | |
| Dysuria | Urinalysis $33 | $184 | |
There was a larger-than-expected variance in the total number of patients between categories (nurse-only 248 and provider 15) because the vast majority of patients that qualify for nurse-only protocol choose that route of care, compared with seeing a provider. Patient contact rates of 63% for nurse-only patients and 71% success for providers, respectively, was achieved. As a whole, the evaluation of quality, satisfaction of care, and cost analysis between nurse-only and provider visits for the chief complaints of isolated sore throats and dysuria presented results that supported the original hypothesis: The nurse-only program at Winona Health Urgent Care does in fact provide patients with a satisfactory and more cost-effective alternative to traditional provider care.
Limitations
This study has several limitations. One is that the study arms were not randomized, but based on patient preference. Patient rationale for selecting an arm of the study was not studied, but could include perceived severity of illness or perceived financial consequences of their choice, injecting variation into the two groups and making comparisons less conclusive. Also, a large majority of patients when given the option chose nurse-only care in our population, making the volume in each arm of the study unequal. Finally, nurses and providers were aware of the study and that follow-up phone calls would be made, perhaps influencing their decision-making and demeanor relative to nonstudy patients.
Conclusion
Exploring new ways in medicine to lower cost while maintaining quality and patient satisfaction are important to a sustainable healthcare system. Protocol-driven care for two basic chief complaints by RNs in this study showed no statistical difference in quality or satisfaction relative to traditional care at a much lower cost to the patient. Total savings to patients from this process in this clinic alone is approximately $600,000 annually.3 Expanding this concept to additional uncomplicated medical complaints is supported by this early success. Patients strongly preferred participating in the nurse-only pathway when offered the option (94%).
We were aware that the nurse-only program was popular, but the strong preference for it over traditional provider based care was surprising. Patients were not directly asked why they preferred nurse-only care, but we would speculate that the lower cost and perceived faster service were motivators. The nurse-only protocols involved in the study have objective laboratory evidence to rely on in medical decision-making. Perhaps this improves the confidence of patients in nurse-only care in these areas, leaving more subjective medical decision-making to those with a higher level of training. However, in this sample, there were no identified patients with an alternative diagnosis identified in follow-up visits. That does pose as a risk, and attempts to mitigate it were made in the inclusion/exclusion criteria of the nurse-only protocol (see Appendix).
{kind=link}
References
- Whyte B. RN visit for pharyngitis (strep throat) and uncomplicated urinary tract infection algorithms. Winona Health. Updated Dec. 28, 2015.
- Centers for Medicare and Medicaid Services. NHE Fact Sheet. Available at: https://www.cms.gov/research-statistics-data-and-systems/statistics-trends-and-reports/nationalhealthexpenddata/nhe-fact-sheet.html. Accessed December 6, 2017.
- Bureau of Labor Statistics. United States Department of Labor. Available at: https://www.bls.gov/.
- Undeland DK, Kowalski TJ, Berth WL, Gundrum MS. Appropriately prescribing antibiotics for patients with pharyngitis: a physician-based approach vs. a nurse-only triage and treatment algorithm. Mayo Clin Proc. 2010;85(11):1011-1015.
- Lean Consulting. Best practice in measuring customer satisfaction. Available at: http://www.leanconsulting.com/resources/best-practice-in-measuring-customer-satisfaction/. Accessed January 15, 2016.
- Winona Health Billing Department. Winona, MN.

Kyle Coon
