Published on
Urgent message: Too often, patients first learn that they have hypertension secondary to an unrelated presenting complaint—often, in the urgent care setting. Improving adherence to treatment guidelines may improve management and, ultimately, outcomes.
Jennifer Iacovo, DNP, APRN, FNP-C; Bonni Cohen, PhDc, DNP, APRN, ANP-C, FNP-C, CHFN, CNE, FAANP; and Judith Butler, DNP, CNM, WHNP, CNE
Abstract
Background: There are approximately 100 million adults in the U. S. with hypertension (HTN); almost half go undiagnosed. The adjusted national cost burden for the treatment of HTN exceeds $130 billion. Early HTN screening and treatment can help avoid unwanted cardiovascular events such as heart attack and stroke. Considering the limited research on HTN management in the urgent care setting, along with varying provider perceptions, the majority of patients leave the urgent care without an evaluation and treatment plan.
Local Problem: Chart audits at an urgent care clinic in the southwest region of the United States revealed that 80% to 100% of clinicians were noncompliant in providing proper HTN management. Further, BP measurements were not uniformly nor accurately performed by the clinic staff.
Objective: To improve the effective management of adult HTN within an urgent care setting over a 90-day period.
Methods: A mixed-methods approach and four rapid plan-do-study-act (PDSA) cycles were used. Throughout the implementation process, data collected from surveys, observations, and chart audits were input into an aggregate data workbook and analyzed through a series of run charts. There were four primary interventions:
- A BP measurement checklist to provide a clinic protocol
- A patient shared decision-making (SDM) tool to increase patient involvement in HTN care
- A clinician adult high BP best practice checklist for adherence with best evidence-based practice (EBP) guidelines
- A team engagement plan to increase team collaboration
Results: Informed by composite scores regarding BP measurement accuracy, adherence to EBP guidelines, and patient HTN comprehension and satisfaction, adult HTN management improved from 28% to 88% in 90 days. Both checklists produced positive outcomes by improving BP measurement accuracy and HTN quality care compliance. The patient SDM tool enhanced overall BP patient comprehension and increased BP management satisfaction with a mean composite score of 94% throughout implementation. Overall, the healthcare team collaboration rose from 55% to exceed the goal of 80%, through a series of team activities.
Discussion: Success in meeting all goals was a direct result of a combination of team and patient engagement strategies, demonstrating the usefulness of the intervention measures in improving effective BP management in an urgent care setting. Screening for undiagnosed HTN in urgent care clinics through the development of specific protocols offers an important opportunity to reduce associated disease burdens.
Citation: Iacovo J, Cohen B, Butler J. Implementing clinical practice guidelines in adults with hypertension: an effective practice change in urgent care.J Urgent Care Med. 2021;15(6):XX-XX.
Jennifer Iacovo, DNP, APRN, FNP-C; Bonni Cohen, PhDc, DNP, APRN, ANP-C, FNP-C, CHFN, CNE, FAANP; and Judith Butler, DNP, CNM, WHNP, CNE
INTRODUCTION
Hypertension (HTN) affects over 100 million U.S. adults and contributes to the leading cause of mortality in our nation, which is heart disease.1, 2 Linked to a number of health disease burdens such as vision loss, renal disease, heart failure, sexual dysfunction, and peripheral artery disease, the annual HTN-associated healthcare costs total approximately $131 billion.3 Perhaps most alarming, approximately half (46%) of those individuals with HTN do not even know it, leaving them at risk for years of damage before symptoms develop.1 With identification of HTN through early screening and treatment, substantial benefits can be recognized and unwanted cardiovascular events can be avoided such as heart attack, stroke, or death.4
Furthermore, there are approximately 90 million reported visits made to the urgent care system each year; statistically, it’s likely that almost half of the adults we come in contact with each day have undiagnosed HTN.5 In the clinician’s perception, elevated BP in the urgent care setting is often thought to be related to pain, anxiety, or white-coat syndrome, with the assumption being that after discharge their BP will normalize.6 This results in a large majority of adult patients with asymptomatic HTN in the urgent care setting not being evaluated and being discharged without a HTN specific plan of care.7 With the declining trend in the percentage of patients having a primary care clinician, the urgent care setting is often viewed as the frontline of healthcare for patients due to its convenient access and cost savings.8,9 It is imperative that this setting engage in the early identification and management of asymptomatic HTN to help reduce overall mortality rates.
LITERATURE REVIEW
There is a paucity of research on the evaluation and management of asymptomatic HTN patients within the urgent care setting. The American College of Cardiology (ACC) and the American Heart Association (AHA) Task Force provides the latest evidence-based HTN recommendations and updated BP categories for medical professionals to follow.10 In addition, the U.S. Preventive Services Task Force (USPSTF) provides HTN screening recommendations for all adults ≥18 years old.4 These guidelines provide strong data-driven support on the screening and management of adult HTN but lack the evidence-based guidance on how to manage these patients within certain specialty settings, such as urgent care.
Although limited, there are some findings on the management of asymptomatic HTN patients in the ED. The American College of Emergency Physicians (ACEP) has a clinical policy on the evaluation and management of asymptomatic HTN patients in the ED, which recommends that patients with asymptomatic, markedly elevated BP be referred for outpatient follow-up.11 Overall, the literature revealed that referral and follow-up for patients who have asymptomatic high BP in the ED setting lacked adherence and was partly due to clinician attitudes and being unfamiliar with the latest guidelines.12 When it comes to screening, a recent study found that patients who had an elevated BP measured in the ED had an increased incident of atherosclerotic cardiovascular disease (ASCVD), heart attack, or stroke by the end of a 6-year follow-up, suggesting the need for further intervention within this type of setting.13 Furthermore, one recent study suggests that the application of a screening, brief intervention, and referral for treatment (SBIRT) model on asymptomatic HTN patients within the ED setting could help encourage early identification and referral for these patients.14 It is reasonable to conclude that similar to the ED, the SBIRT model can be applied to patients in the urgent care setting. This initiative examined how the latest HTN guidelines were implemented in an urgent care setting and to further explore potential gaps in HTN management.
RATIONALE AND OBJECTIVE
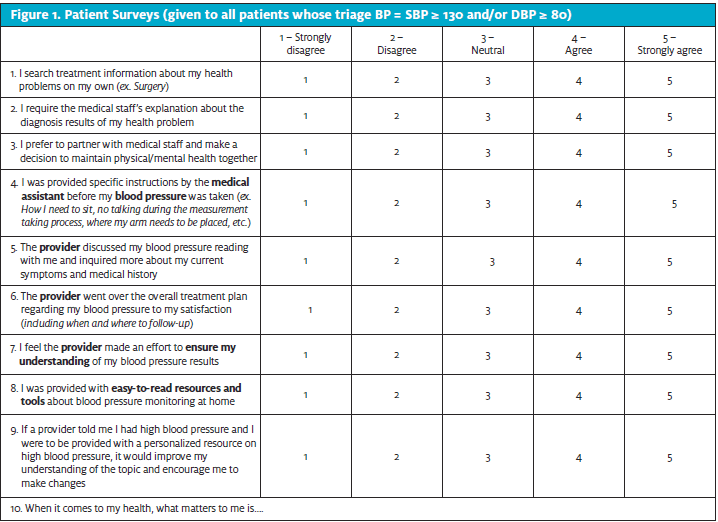
An initial root cause analysis was performed to help identify gaps in HTN care at an urgent care clinic in the southwest region of the United States. When compared to the latest 2017 ACC/AHA HTN guidelines, evaluation of the BP measurement process revealed that staff were missing critical elements in performing an accurate BP measurement with each patient encounter. In addition, for those patients who had a systolic BP of ≥ 130 and/or diastolic BP ≥ 80 (HTN Stage I) measured in clinic, pre-intervention patient surveys (n=20) (Figure 1) revealed that BP readings were not being addressed by the clinician in 80% of visits, indicating a lack of quality in care. Furthermore, a randomized chart review of adult patients (n=40) who had a systolic BP of ≥ 130 and/or diastolic BP ≥ 80 (HTN Stage I) or higher was conducted between February 1, 2019 and March 31, 2019 revealed that 80% to 100% of charts were noncompliant in following best practice guidelines through repeating an elevated BP reading, utilizing proper diagnosis codes, and providing HTN education and specific follow-up instructions. Of note, patients’ BP fell within HTN stage II BP category (SBP ≥ 140 and/or DBP ≥ 90) in 98% of charts reviewed. Together, these findings reveal a gap in HTN quality care in the urgent care setting and the further need to improve the management of these patients through a quality improvement (QI) study. For this reason, the implementation of QI strategies aimed to improve the effective management of adult high blood pressure in an urgent care setting from 28% to 60% over the course of 90 days.
METHODS
Study Setting and Inclusion Criteria
This QI study was implemented at an urgent care clinic in south-central Arizona. Patient population is drawn from a large metropolitan area primarily of Caucasian (54%), Hispanic (31%), and African American (6%) ethnicity with an uninsured rate of 13% and poverty level of 12%.15 Averaging approximately 35 visits per day, the project site operates each shift with one medical clinician, one back office medical assistant, and one front office representative. Inclusion criteria included all adult patients ≥ 18 years old who presented to the clinic for an urgent care visit between July 15, 2019 to September 8, 2019 on most days of the week while participating staff was working. The Institutional Review Board (IRB) approved this initiative as excused, meeting federal requirements for a quality improvement project. Additionally, no outside funding was received.
Design
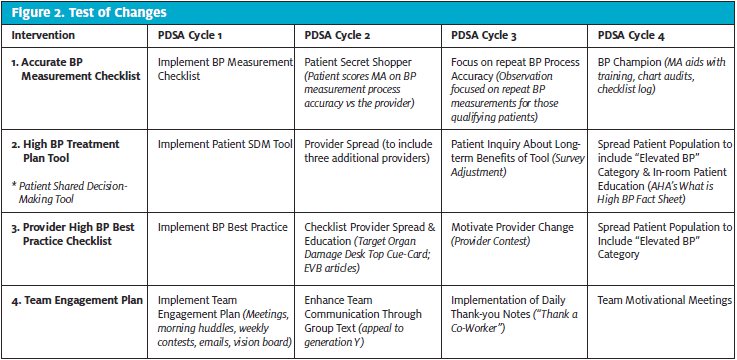
In line with the Institute of Healthcare Improvement (IHI) recommendations, this initiative followed four plan-do-study-act (PDSA) cycles, which provided a model for improvement for testing small scale changes before broader implementation.16 Each of the PDSA cycles lasted two weeks to allow for rapid cycle improvements over an eight week period. Small tests of changes (TOCs) were applied towards four core interventional tools (CITs) based on data from the previous cycle (Figure 2). A mixed methods approach consisting of both qualitative and quantitative methodologies were used to allow for a more in-depth evaluation of the four CITs. Through the use of quantitative methodology, a retrospective chart review, surveys, and observational tools were performed at baseline and every 3 days. Data was input into an aggregate Excel workbook and analyzed using run charts, which allowed for immediate quality improvements. Qualitative data was gathered from staff and patients’ feedback throughout the implementation process and observed for any recurring themes.
Interventions
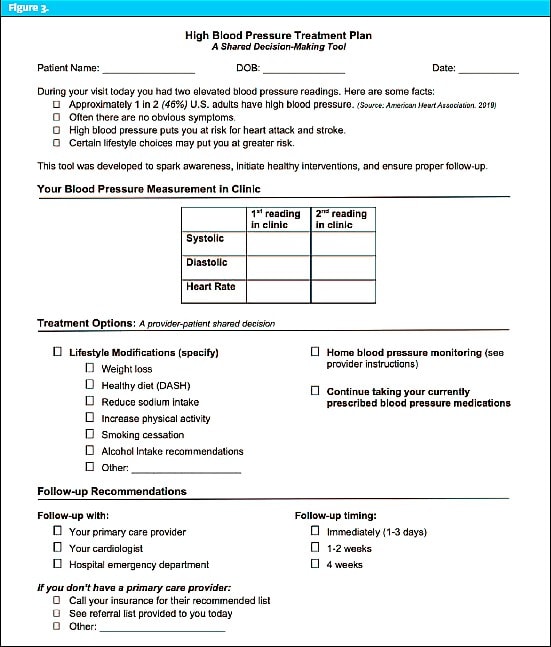
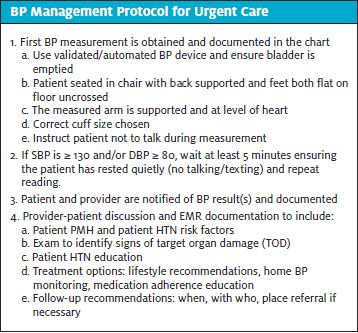
There were four CITs utilized throughout this study that were adapted from existing evidence-based practice guidelines, checklists, and toolkits. The first intervention was a BP measurement checklist that was laminated and attached to each vital sign monitor to effectively aid MAs with BP measurement accuracy. The second, a patient shared decision-making (SDM) tool, the High BP Treatment Plan (Figure 3), followed a SBIRT model approach and explained HTN risks and treatment recommendations according to the latest guidelines. The SDM tool was initiated by the MAs during the triage process for patients with a HTN Stage I BP measurement or higher and then given to the clinician to facilitate a bidirectional BP discussion. All identified patients were given a survey at the end of their visit to evaluate their overall satisfaction and comprehension of their BP results. The third tool is the clinician High BP Best Practice Checklist, which also followed a SBIRT model approach and consisted of evidence-based HTN recommendations to improve chart compliance. Finally, a team engagement plan that included meetings, huddles, vision boards, and weekly contests, were scheduled to enhance team collaboration throughout the QI process. At the end of each cycle the healthcare team received a survey to assess for changes in team confidence, accountability, attitudes, communication, and support.
Measures
To help identify areas of improvement, ten measures were developed, including a balancing measure and aim, along with corresponding operational definitions. Each of the four CITs implemented utilization rates for their process measures through the use of a daily log system. Outcomes measures for each of the four CIT’s were obtained through the use of individualized scoring tools. The outcome measures for both checklists were determined through mean scores obtained from observation of the BP measurement taking process (BP accuracy score) and chart audit reviews (HTN best practice score). In addition, mean scores were also taken from weekly patient and team surveys (Patient BP comprehension/satisfaction score and team collaboration score) that used a 5-point Likert scale to determine outcome measure results for those instruments.
Data Analysis
To study the impact of the four CIT’s, quantitative data was plotted on run charts and analyzed weekly to identify variations, trends, and shifts in the process during implementation, which helped to identify process improvement or degradation over time.17 Qualitative data collected through field notes along with patient and staff open-ended questions were evaluated weekly for any recurring themes to gain insight on how they impacted the measures. Throughout implementation, in-person ongoing evaluation of contextual elements were performed to ensure that the information obtained was reliable and valid for completeness and data accuracy.
RESULTS
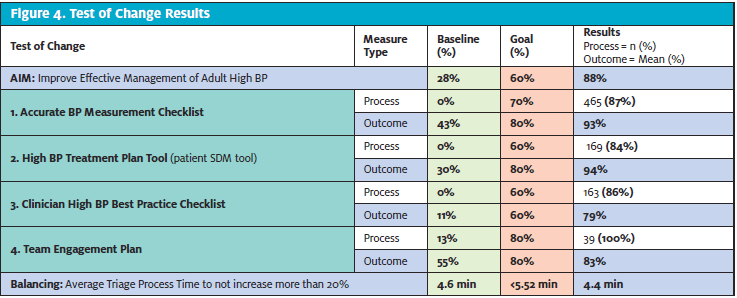
The four CITs produced positive process and outcome measure results, surpassing all goals by the end of the rapid four PDSA cycles (Figure 4). The effective management of HTN in adults in an urgent care setting improved from 28% to 88%, exceeding its goal of 60%. Effective HTN management was accomplished by improving BP measurement accuracy, adherence to EBP guidelines, and patient HTN comprehension and satisfaction. An unintended consequence of the initiative yielded a 4.35% improvement in the triage process time by the end of initiative completion.
Implementation of a BP Measurement Checklist
The BP measurement checklist was utilized in a total of 465 patients, improving staff BP measurement technique from 43% to 93% in 90 days. In PDSA cycle 1, staff training improved BP measurement accuracy from a baseline of 43% to 91%. PDSA cycle 2 incorporated a secret shopper which further validated the BP measurement process and ensured that reliable data were collected. To assess the sustainability of the checklist process and desired outcomes, a BP champion was added during PDSA cycle 4 to place leadership responsibility on the MA and to test sustainability. This small TOC demonstrated to be beneficial by contributing to a final BP accuracy mean score of 94%, surpassing the goal of 80%.
Patient Engagement
Over the course of the study, 84% of patients whose BP met HTN Stage I or higher criteria (ACC/AHA, 2017) received HTN specific education with the clinician. Use of the patient SDM tool (Figure 3) resulted in immediate improvement in patient satisfaction and comprehension of their BP results from 30% to 97% during PDSA cycle 1. As predicted, during PDSA cycle 2, the addition of a second clinician decreased tool utilization rates from 90% to 78%; however, patient satisfaction and understanding of their BP measurement remained high at 97%. During cycle 3, the patient survey was revised to inquire about the long-term benefits of BP discussion in a specialty setting. While utilization remained at 89%, 75% of patients stated that the BP discussion would have a positive effect on their long-term health. Cycle 4 increased patient eligibility to include those patients whose BP fell within systolic 120-129 (elevated BP category).10 This resulted in a 3% decrease in survey scores, still contributing to an overall survey mean of 94% and exceeding the goal of 80%.
Implementation of a High BP Best Practice Checklist
A guideline-driven High BP Best Practice Checklist was made available for clinicians to use next to the charting station, resulting in a total of 163 checklists used throughout implementation and improvement in HTN chart audit rates from 11% to 80%. After expanding the checklist to include additional clinicians during PDSA cycle 2, there was a predicted initial drop in chart audit compliance with aggregate data identifying target organ damage (TOD) documentation as one of the lowest quality measures. To help improve HTN documentation the use of a TOD desktop cue card was implemented, improving TOD documentation from 43% to 68% by the end of PDSA cycle 3. In PDSA cycle 4, expanding the patient population to include BP measurements that fell within the 2017 ACC/AHA elevated BP category (systolic BP of 120-129 and/or diastolic BP <80) resulted in a decrease in chart audit scores from 89% to 80%. With an overall tool utilization median of 88%, a direct correlation was made between tool utilization and expected outcomes, exceeding both goals of 60%.
Team Engagement
The launch of the team engagement plan during PDSA cycle 1 resulted in a steady upward trend in team encounters throughout implementation and had a positive correlation with overall team collaboration survey scores, which looked at the overall attitudes, confidence, accountability, support and communication of the team. To enhance team support and communication methods, the addition of a team group text during cycle 2 and daily shift thank-you cards during cycle 3 were implemented, which proved to be effective in improving team survey scores from 55% to 88%. To help improve team collaboration scores during cycle 4, motivational meetings with each team member were unsuccessfully attempted due to time constraints, which resulted in a 1% decrease from previous cycle survey averages, still exceeding our goal of 80% at the end. The team engagement plan concluded with the completion of 100% of team encounters, with team collaboration scores improving from 55% to 87% by the end of PDSA cycle 4.
DISCUSSION
Team collaboration improved the management of adult HTN in the urgent care setting from 28% to 88%, indicating the usefulness of all four CIT’s in improving HTN care. The use of checklists, composed of evidence-based practice guidelines, demonstrated to be an effective approach in ensuring patient safety and quality improvement.18 Specifically, the BP measurement checklist improved efficiency and validity of the measurement-taking process, with an unexpected outcome in improving triage process times. The use of the clinician-driven HTN best practice checklist improved outcomes in HTN quality of care and charting compliance. Finally, the use of the SBIRT model was highly effective in identifying and intervening in the care of hypertensive patients within the urgent care setting providing the ability to close health disparity gaps for this population.
Most importantly, the direct involvement of patients with the use of a patient SDM tool helped to initiate discussion and patient involvement with HTN care while in the fast-paced environment of the urgent care setting. This was associated with improvement of HTN care and enhanced patient understanding of their BP results. Patients want and need to be involved in their care, as it can lead to measurable advances in safety and quality compliance.19 The SDM tool provided a positive impact on the urgent care system and patient population, and it would be feasible to spread the use of this tool by placing it in the electronic health record (EHR) system, similar to the Bartels et al. (2017) BP Connect toolkit.20 Similarly, the development of the team engagement plan that encompassed a variety of activities and communication methods was associated with the effective utilization of all tools and improved patient and clinician outcomes. Employees play a vital role in driving the success of the organization and through the use of workforce engagement, employee productivity and performance were enhanced.21 Without the high level of commitment from the staff, the results could have shown continued gaps in HTN management but ultimately the effort resulted in positive patient and data trends, as well as the overall success of this QI study.
LIMITATIONS
This study was conducted at one site in an urban community during the summer months. This limits generalizability to other urgent and retail clinics in different community locations that have a fluctuating patient census. Although modified from existing tools, none of the tools utilized were validated, which therefore limits the validity of the results. In addition, the difficulty of patient follow-up within the urgent care setting led to the assumption that patients would adhere to clinician recommendations and seek follow-up care with their primary care clinician or cardiologist. Recommendations to mitigate these limitations include using a larger sample size with a more diverse population and performing patient follow-up calls.
CONCLUSION
Over the course of 90 days, the effective management of adult HTN in the urgent setting improved through the guidance and direction of a clinician-led initiative. More importantly, its success in meeting all goals was a direct result of a combination of team and patient engagement strategies. Screening for undiagnosed HTN in the urgent care clinics offers an important opportunity to reduce the associated disease burden while helping to combat our nation’s leading cause of death – heart disease. This study has significance for local and national systems as its tools provided a simple and inexpensive method to provide accurate BP screening, brief interventions, and follow-up recommendations within a specialty setting, allowing for easy replication into any healthcare facility that uses vital signs. Future project sustainability can be maintained through the development of a company-wide protocol and transitioning the tools into the EHR while also promoting its use at other sites. Further research is recommended to determine the long-term impact that the four CITs have on overall patient cardiovascular health.
References
- American Heart Association. More than 100 million Americans have high blood pressure, AHA says. American Heart Association. Available at: https://www.heart.org/en/news/2018/05/01/more-than-100-million-americans-have-high-blood-pressure-aha-says. Published January 31, 2018. Accessed March 4, 2020.
- Centers for Disease Control and Prevention. Leading causes of death. CDC. Available at: https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm. Last Reviewed March 2017. Accessed March 4, 2020.
- Kirkland EB, Heincelman M, Bishu KG, et al. Trends in healthcare expenditures among US adults with hypertension: national estimates, 2003-2014. J Am Heart Assoc. 2018;7(11): 1-9.
- U.S. Preventative Service Task Force. Screening for high blood pressure in adults: U.S. preventive services task force recommendation statement. Ann Intern Med. 2015;163(10):778-786.
- Dolan S. The urgent care industry trends looking to fulfill the demand of a growing segment in the healthcare market. Urgent Care Association. Available at: https://www.ucaoa.org/About-UCA/Industry-News/ArtMID/10309/ArticleID/950/The-urgent-care-industry-trends-looking-to-fulfill-the-demand-of-a-growing-segment-in-the-healthcare-market. Accessed March 4, 2020.
- Armitage LC, Whelan ME, Watkinson PJ, Farmer AJ. Screening for hypertension using emergency department blood pressure measurements can identify patients with undiagnosed hypertension: a systematic review with meta-analysis. J Clin Hypertens. 2019; 21(9):1415-1425.
- Karras DJ, Kruus LK, Cienki JJ, et al. Evaluation and treatment of patients with severely elevated blood pressure in academic emergency departments: a multicenter initiative. Ann Emerg Med. 2006;47(3):230-236.
- American Academy of Urgent Care Medicine. What is urgent care medicine? AAUCM. Available at: https://aaucm.org/what-is-urgent-care-medicine/. Accessed March 4, 2020.
- Levine, DM Linder JA, Landon BE. Characteristics of Americans with primary care and changes over time, 2002-2015. JAMA Intern Med. 2020; 180(3):463-466.
- Whelton PK, Carey RM, Aronow WS, et al. ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults. J Am Coll Cardiol. 2018;71(19):e127-e248.
- Wolf SJ, Lo B, Shih RD, et al. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Intern Med. 2015; 62(1):59-68.
- Souffront K, Chyun D, Kovner C, Ogedegbe O. Barriers and facilitators to referral for asymptomatic hypertension in the emergency department: a multidisciplinary survey of ED providers in the U.S. J Hypertens Manag. 2016;2(1):1-8.
- Oras P, Habel H, Skoglund PH, Svensson P. Elevated blood pressure in the emergency department: A risk factor for incident cardiovascular disease. Hypertension.2019;75(1): 229-236.
- Pirotte MJ, Buckley BA, Lerhmann JF, Tanabe P. Development of a screening and brief intervention and referral for treatment for ED patients at risk for undiagnosed hypertension: A qualitative initiative. J Emerg Nurs. 2014;40(1):1-9.
- United States Census Bureau. QuickFacts: Maricopa County, Arizona. United States Census Bureau. Available at: https://www.census.gov/quickfacts/fact/table/maricopacountyarizona/PST045219. Accessed March 4, 2020.
- Langley GL, Moen R, Nolan, KM, et al. The improvement guide: A practical approach to enhancing organizational performance (2nd ed.). San Francisco, CA: Jossey-Bass Publishers; 2009.
- Ogrinc GS, Headrick LA, Barton AJ, et al. Fundamentals of healthcare improvement: A guide to improving your patients’ care (3rd ed.). Oak Brook, IL: Joint Commission Resources; 2018.
- Sligo J, Roberts V, Gauld R, et al. A checklist for healthcare organizations undergoing transformational change associated with large-scale health information systems implementation. HPT. 2019;8(3):237-247.
- Agency for Healthcare Research and Quality. Guide to improving patient safety in primary care setting by engaging patients and families. AHRQ. Available at: https://www.ahrq.gov/patient-safety/reports/engage.html. Accessed March 4, 2020.
- Bartels C, Ramly E, Panyard D, et al. BP connect toolkit: a specialty staff protocol to improve follow-up after high blood pressures. HIPxChange. 2017. Available at: https://www.hipxchange.org/BPConnect. Accessed March 4, 2020.
- Burton WN, Chen CY, Li X, Schultz AB. The association of employee engagement at work with health risks and presenteeism. J Occup Environ Med. 2017;10:988-992.
Author affiliations: Jennifer Iacovo, DNP, APRN, FNP-C, HonorHealth FastMed Urgent Care, Arizona. Bonni Cohen, PhDc, DNP, APRN, ANP-C, FNP-C, CHFN, CNE, FAANP, Valdosta State University College of Nursing. Judith Butler, DNP, CNM, WHNP, CNE, Frontier Nursing University. The authors have no relevant financial relationships with any commercial interests.