Published on
Urgent message: Typical drooling is no cause for alarm in infants and toddlers. However, excessive drooling accompanied by fever or other various red flags could be signs of more serious concerns such as retropharyngeal abscess, Ludwig angina, or upper airway obstruction. Recognition should trigger a thorough evaluation by the urgent care provider.
Katherine P. Dureau, MD
CASE
A 24-month-old previously full-term and vaccinated male presents to an urgent care center with 24 hours of fever with a maximum temperature of 102.5⁰F. The father also reports drooling, decreased oral intake, fussiness, and with no urine output for 12 hours. There is associated diaper rash, congestion, and rhinorrhea but no neck stiffness, neck swelling, or difficulty breathing. The child goes to daycare and has two older school-aged siblings.
On examination, the patient is fussy but nontoxic appearing and in no respiratory distress. He is febrile to 102.2⁰F with a heart rate of 140 beats/minute and a respiratory rate of 32 breaths/minute. He is irritable but consoles well to the father. He has normal range of motion of his neck without a palpable mass. He has copious clear drooling from the mouth.
INTRODUCTION
It is normal for infants and toddlers to drool as part of their oral-motor development, as well as with the eruption of new teeth. However, excessive drooling coupled with fever or an ill appearance should prompt the urgent care clinician to perform a thorough examination of the head and neck, placing special emphasis on the mouth and oral cavity. Visualization of the oral mucosa can help distinguish benign and self-limiting illnesses from acute and life-threatening emergencies.
HISTORY AND EXAM PEARLS
The majority of the diagnoses that include fever and drooling can be made clinically, often without the need for additional laboratory testing or imaging.
Inquire about prodromal symptoms including nasal congestion, chest congestion, coryza, cough, emesis, and diarrhea which may suggest a viral etiology. Other factors to ascertain include change in voice, refusal to eat, dysphagia, sore throat, trismus, neck pain, neck stiffness, and difficulty breathing.
A child who is up to date on their immunizations has protection against vaccine-preventable illnesses such as epiglottitis and diphtheria. A series of DTaP and Hib vaccines is recommended starting at 2 months old to protect against the aforementioned diseases commonly caused by H influenzae type B and C diphtheriae, respectively.
The examination should begin by noting the general appearance of the child. An ill-appearing child is more suggestive of a bacterial etiology, including retropharyngeal abscess, Ludwig angina, and epiglottitis. Stridor and/or neck extension are suggestive of upper airway obstruction. Children with lesions causing glottic narrowing such as epiglottitis or deep neck infection classically prefer to sit up in the “tripod” or “sniffing position” to maximize airway patency.
Though it may be difficult in a fussy child, valuable information can be discovered by visualization of the tongue, buccal mucosa, soft and hard palate, gingival ridge, uvula, posterior pharynx, and tonsils in addition to the neck and cervical area.
Specific findings may include:
- The presence of neck swelling and stiffness in conjunction with drooling and fever which may be suggestive of a deep neck infection.
- Tenderness, erythema, and fluctuance of the submandibular area are suggestive of Ludwig angina.
- White plaques on the buccal mucosa, palate, tongue, or the oropharynx are characteristic of oral candidiasis (thrush).
- Oral ulcers are the hallmark of hand-foot-and-mouth disease (HFMD), herpangina, and herpes gingivostomatitis, with the location of these lesions within the mouth being the clue to distinguishing one from the other.
- The lesions of HFMD and herpangina are typically located in the posterior mouth, including the soft palate, tonsils, and uvula.
- Herpes gingivostomatitis commonly involves the anterior oral cavity, lips, and skin around the mouth. The affected mucosa appears friable, erythematous, and edematous.
- Herpes stomatitis has a more insidious onset and longer duration. HFMD and herpangina mostly occur in the summer and early fall, whereas herpes stomatitis occurs year-round.
A gentle approach should be taken when examining the mouth, as the aforementioned lesions can be quite painful to touch.
Suspected herpangina

Credit: Katherine P. Dureau, MD
In addition to the oral exam, perform a skin assessment, paying particular attention the palms, soles, and diaper area as HFMD and other enterovirus variants may be characterized by a vesiculopapular rash in these areas. Involvement of the buttocks and genital area occur in 30% of cases.1
| Differential Diagnosis | |
| What’s Common | · Hand, foot, and mouth disease· Herpangina
· Herpes gingivostomatitis · Thrush · Streptococcal/viral pharyngitis & tonsillitis |
| What Not to Miss | · Retropharyngeal abscess· Ludwig angina |
| What to Think About | · Epiglottitis |
DIAGNOSIS AND MANAGEMENT
What’s Common
- The diagnosis of HFMD and herpangina is made with the identification of ulcers on the posterior oropharynx. These illnesses are commonly caused by the Coxsackie virus (an enterovirus). When ulcers are isolated to the mouth, it is called herpangina. When coupled with lesions on the palms or soles, it is referred to as hand-foot-and-mouth. Some variants (eg, Coxsackie A6) are characterized by more diffuse rash, particularly around the mouth and on the buttocks. The illness begins with the sudden onset of high fever along with the eruption of painful oral lesions.2-4 Management includes supportive care with antipyretics and pain relievers, as the illness is usually benign and self-limited. Reinforce adequate hydration; a mouthwash containing equal parts Maalox and Benadryl may help soothe oral discomfort, but data proving its efficacy are lacking.5
- Herpes gingivostomatitis is the most common manifestation of a primary herpes simplex virus (HSV) infection of childhood. It is characterized by the onset of prodromal symptoms including fever, irritability, and malaise followed by the eruption of painful mucocutaneous vesicular lesions. Relative to the Coxsackie viruses, HSV-1 more typically causes ulcers in the anterior oral area (eg, gingiva, tongue, and lips). Classic skin lesions around the lips are vesicles that often cluster together and coalesce. The gingiva appear inflamed and bleed easily.6,7 The diagnosis can be made clinically without the use of additional laboratory techniques to confirm the diagnosis; however, sending a viral PCR test may be necessary in children who are immunocompromised as the risk of complications may be higher. Oral acyclovir may help shorten the duration of symptoms if initiated within 72-96 hours of disease onset.5 Keep in mind that neonates concerning for cutaneous HSV infection require special consideration for escalation of care due to the high risk of morbidity and mortality associated with HSV encephalitis and disseminated infections in this particular population.
- Thrush is an oropharyngeal Candida infection that is common in healthy infants. It is manifested as white plaques on the intraoral mucosa. Milk curd can be difficult to distinguish from thrush; a trick is to run a tongue depressor over the plaques, as thrush is difficult to remove. Treatment is with topical nystatin suspension.8 Thrush does not typically cause a fever, although some infants could have a coexisting viral infection that causes elevation in body temperature.
- Acute bacterial pharyngitis is most commonly due to a group A streptococcus (GAS) infection. It affects children ages 5─15 years old. Clinical manifestations include fever and sore throat and, when severe, can be associated with difficulty swallowing. On exam, the tonsils are enlarged and erythematous, with or without exudates. Cervical lymphadenopathy is often present. Ill appearance, neck stiffness, and trismus are not typically associated with uncomplicated tonsillopharyngitis. Viruses predominate as acute infectious causes of tonsillopharyngitis and often mimic the symptoms and exam findings of GAS pharyngitis. The treatment is supportive for viral causes; however, GAS pharyngitis requires antibiotic therapy.15
- As opposed to common viral illnesses that present with fever and drooling, children with deep neck infections usually have a more dramatic presentation including ill appearance, refusal to move the neck, and, rarely, stridor.
What Not to Miss
- A retropharyngeal abscess (RPA) is a deep neck space infection that presents in children <6 years old, peaking at age 3 years. Serum evaluation may show a leukocytosis with left shift, sometimes with a thrombocytosis and elevation of inflammatory markers (ESR, CRP), however these findings are nonspecific. A lateral neck radiograph may show increased depth in the prevertebral space on lateral radiograph suggesting a space-occupying lesion between the esophagus and vertebral column. However, immediate transfer to the ED may be preferable to taking the time to perform an x-ray, especially if the child shows signs of respiratory distress or there is a high clinical suspicion. If the clinician does opt for lateral neck imaging on site, the film should be taken during inspiration and false thickening can be caused by crying, especially in infants. Prevertebral space thickening on a good quality film has fair specificity for an RPA, but a negative film does not exclude the possibility of a deep neck infection. In addition, this is not a definitive study to guide management. Contrast-enhanced neck CT is the imaging modality of choice to identify, localize, and differentiate abscess from phlegmon/cellulitis. Signs of an RPA should prompt referral to a specialty center for further evaluation by a pediatric otolaryngologist, as management includes intravenous antibiotic therapy and possible surgical intervention.9,10
Child with normal prevertebral space
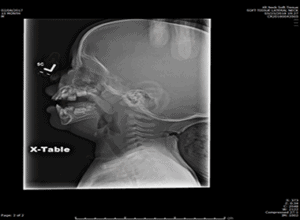
Credit: Neil Vachhani, MD, Children’s Hospital of the King’s Daughters, Norfolk VA
Child with prevertebral space widening
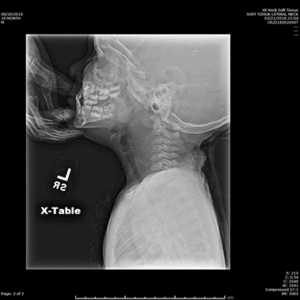
Credit: Neil Vachhani, MD, Children’s Hospital of the King’s Daughters, Norfolk VA
Note arrow indicating prevertebral space widening

Credit: Neil Vachhani, MD, Children’s Hospital of the King’s Daughters, Norfolk VA
- Ludwig angina (submandibular space infection) is a bacterial cellulitis of the floor of the mouth in the sublingual and submaxillary space. In the most severe cases, oropharyngeal intubation is difficult because of the inability to lift the tongue, making this infection a potential airway emergency. Ludwig angina is typically a mixed anaerobic bacterial infection that is often due to spreading of a mandibular molar abscess. Patients present with fever, mouth pain, stiff neck, drooling, and dysphagia. They have tenderness in the submandibular area and the mouth is held open by lingual swelling. The diagnosis is made based on the suggestive exam findings. CT imaging may be helpful to evaluate the depth and size of the infected area. The treatment is empiric broad-spectrum antibiotics, but surgery is usually not necessary. Immediate transport to a specialty center is indicated given the risk of airway compromise from glottic swelling.11,12
What to Think About:
- Epiglottitis is an inflammation of the epiglottis that can lead to a rapidly progressive upper airway obstruction. With the introduction of the Haemophilus influenza type b vaccine, the incidence has dropped dramatically; however, the epidemiology has changed with an increasing incidence secondary to Streptococcus infection in older vaccinated children. Classic epiglottitis should be suspected in an unimmunized toddler with an acute onset of fever, dysphagia, drooling, and respiratory distress. The child may appear toxic and prefer to sit in the “sniffing” or “tripod” position to maximize airway patency. Stridor may also be present, but cough is distinctly uncommon, differentiating epiglottitis from tracheal diseases such as croup and bacterial tracheitis. A lateral neck radiograph may show the classic “thumb sign” demonstrating a swelling of the epiglottis. If the diagnosis of epiglottitis is suspected, immediate transport to a specialty center is indicated and additional stresses should be avoided to prevent the risk of sudden airway obstruction.13,14
CASE CONCLUSION
Upon further examination, the patient’s oral exam shows multiple erythematous oral ulcers on his soft palate. He has scattered erythematous macules on his palms and soles. Removal of his diaper reveals erythematous papules and vesicular lesions. The patient is diagnosed with hand-foot-and mouth disease based on the findings of oral ulcers coupled with skin lesions found on the palms, soles, and buttock. His history and physical examination are absent for red flags to suggest a deep neck space infection or a bacterial infection of the floor of the mouth or epiglottis.
He is given a dose of ibuprofen and a popsicle. Reexamination 30 minutes later shows a playful child without drooling. He appears comfortable and well hydrated. No diagnostic testing is performed. He is discharged home with education and supportive care including acetaminophen or ibuprofen as needed for fever reduction and pain control. Return precautions were discussed, including dehydration or inability to manage pain at home.
Dureau KP. Approach to fever and drooling in infants and toddlers. J Urgent Care Med. July 2018. Available at: https://www.jucm.com/approach-to-fever-and-drooling-in-infants-and-toddlers/.
References
- Hardy E. Hand-foot-mouth disease. Ferri’s Clinical Advisor 2018. 1st ed. Philadelphia, PA: Elsevier; 2018:540.
- Centers for Disease Control and Prevention (CDC). Severe hand, foot, and mouth disease associated with Coxsackievirus A6–Alabama, Connecticut, California, and Nevada, November 2011-February 2012. MMWR Morb Mortal Wkly Rep. 2012;61:213-214.
- Abzug MJ. Hand foot and mouth disease and herpangina. Nelson Textbook of Pediatrics. 20th ed. Philadelphia, PA: Elsevier; 2016:1561-568.
- Michaels MG, Williams JV. Coxsackievirus and other enteroviruses. Zitelli and Davis’ Atlas of Pediatric Physical Diagnosis. 7th ed. Philadelphia, PA: Elsevier; 2018:455-509.
- Faden H. Management of primary herpetic gingivostomatitis in young children. Pediatr Emerg Care. 2006;22:268-269.
- Cohen BA. Herpes simplex virus. Pediatric Dermatology. 4th ed. Philadelphia, PA: Elsevier; 2013:104-125.
- Schiffer JT, Corey L. Therapy for HSV Infections. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 8th ed. Philadelphia, PA: Saunders; 2015:1713-1730.
- Marcdante KJ, Kliegman RM. Oral Cavity. Nelson Essentials of Pediatrics. 7th ed. Philadelphia, PA: Saunders; 2015:429–430.
- Pappas DE, Hendley JO. Retropharyngeal abscess, lateral pharyngeal (parapharyngeal) abscess, and peritonsillar cellulitis/abscess. Nelson Textbook of Pediatrics. 20th ed. Philadelphia, PA: Elsevier; 2016:2021-2023.
- Rose E. Pediatric respiratory emergencies: upper airway obstruction and infections. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 9th ed. Philadelphia, PA: Elsevier; 2018:2069-2080.
- Marcdante KH, Kliegman RM. Pharyngitis. Nelson Essentials of Pediatrics. 7th ed. Philadelphia, PA: Saunders; 2015:347–349.
- Shaw J. Infections of the oral cavity. Principles and Practice of Pediatric Infectious Diseases. 5th ed. Philadelphia, PA: Elsevier; 2018:193-199.
- Marcdante K, Kliegman RM. Croup (Laryngotracheobronchitis). Nelson Essentials of Pediatrics. 7th ed. Philadelphia, PA: Saunders; 2015:354–356.
- Nayak JL, Weinberg GA. Epiglottitis. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, Updated Edition. 8th ed. Philadelphia, PA: Saunders; 2015: 785-788.
- Yellon RF, Chi DH. Otolaryngology. Zitelli and Davis’ Atlas of Pediatric Physical Diagnosis. 7th ed. Philadelphia, PA: Elsevier; 2018:868–915.
Katherine P. Dureau, MD is a board-certified general pediatrician and Fellow, PGY4, in Pediatric Urgent Care, Department of Pediatrics, Division of Emergency Medicine, at Emory University. The author has no relevant financial relationships with any commercial interests
