Published on
Urgent message: Burn injuries present with varying degrees of involvement and severity. It is vital that providers in an urgent care facility understand burn classification, treatments, and, most important, which burn patients can be treated in an outpatient setting and which patients require a higher level of care.
DREW LONG, BS, BRIT LONG, MD, and ALEX KOYFMAN, MD
Introduction
Burn injuries are often devastating and are a leading cause of accidental injury and trauma in both pediatric and adult patients in the United States. Each year nearly 1 million people in the United States seek medical care for burn injuries.1 Although most of these can be treated on an outpatient basis, severe burns can result in significant morbidity and mortality even with hospitalization and adequate treatment.
Several methods of classifying burn injuries may be used to determine burn severity, all of which involve burn size and depth. It is essential that providers in an urgent care setting understand how to classify various burns injuries and to know which patients can be treated at the urgent care center and which patients should be transferred to an emergency department or burn center.
Case Presentation
A 62-year-old woman presents to the urgent care center with scald burns to both forearms. The patient states that she was cooking dinner when a fire erupted. In trying to extinguish the fire, she sustained partial-thickness burns to both forearms. The patient quickly doused her arms in cold water. She decided to come to the urgent care clinic because her blisters were enlarging and painful.
The nurse hands the physician a set of vital signs, all normal. What medical history is important to gather? What is important in the physical examination? How is burn surface area calculated? What areas are high risk? What treatments are beneficial? What injuries meet transfer criteria?
Background
Burns can be devastating injuries from a physical, emotional, and social aspect. A burn is defined as an injury to the skin or other tissue caused by thermal or other exposures. Burns are classified by their depth and size and are broken into minor, moderate, and major. Most of the more than 1 million burns that occur annually in the United States are minor and can be managed in an outpatient setting.1
Burns involve a dynamic process and occur because of skin structural and cellular damage (e.g., from heat, electricity, radiation). Damaged layers of the skin can include the outer, superficial layer of the skin, the epidermis, and the inner layer, the dermis. The epidermis functions as a barrier to the outside world to protect the body from such things as dehydration, microbes, ultraviolet radiation, and heat. The dermis provides strength to the skin and contains blood vessels, hair follicles, sweat glands, and nerves. Injury due to a burn can be divided into three zones: coagulation, stasis, and hyperemia. The zone of coagulation is the point of maximal tissue damage. Decreased tissue perfusion affects the zone of stasis, but injury is potentially reversible with restored perfusion. Inadequate or delay in fluids, infection, or edema can result in complete tissue loss in this area. The outermost region is the zone of hyperemia, which is erythematous because of increased perfusion and release of vasoactive substances. This zone typically heals with no deficits.2,3
Classification
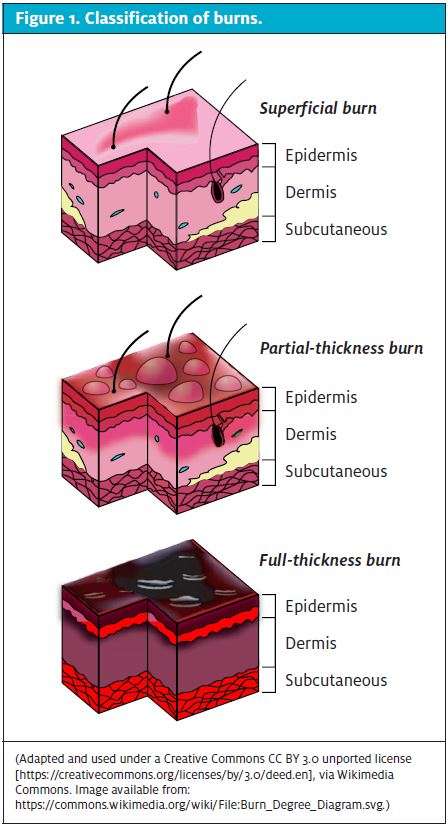
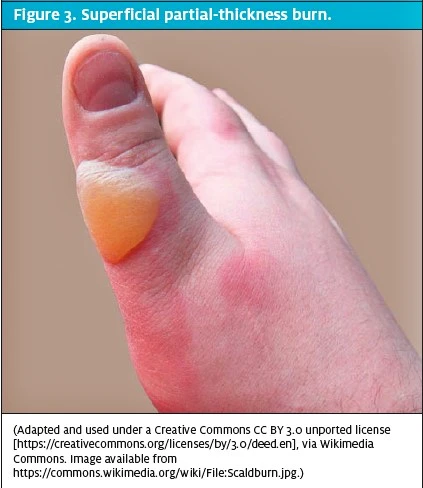
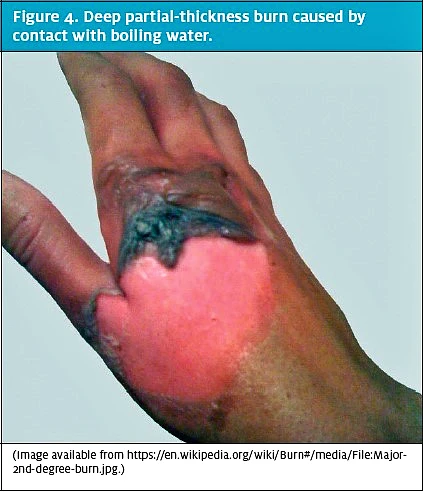
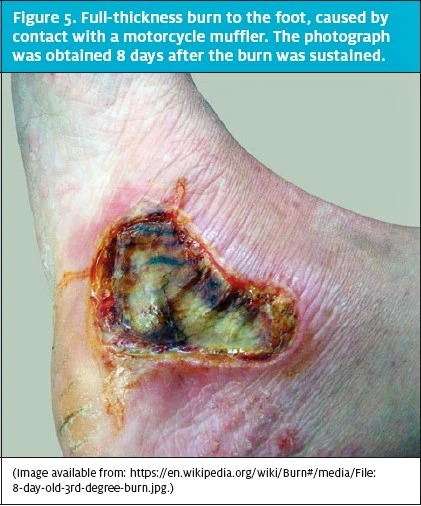
Superficial (first-degree) burns involve the epidermis and are red, flat, painful, and blanch with pressure (Figure 2). These typically heal within 2 to 3 days. Partialthickness (second-degree) burns involve all of the epidermis and part of the dermis (Figure 3). These are further classified into the degree of dermal involvement. Superficial dermal burns involve the entire epidermis and part of the dermis, appear erythematous with clear blisters, are painful, blanch, and typically heal within 2 to 3 weeks. Deep dermal burns involve the entire epidermis and extend into the deep dermis (Figure 4). They involve blistering and appear mottled pink and white, are less painful (because of nerve injury within the deeper dermis), and do not blanch. Full-thickness (third-degree) burns involve the entire epidermis and dermis (Figure 5). The appearance of full-thickness burns can range from white to black. These burns are insensate and nonblanching. Fourth-degree burns extend into the underlying adipose tissue, muscle, and bone.2,3
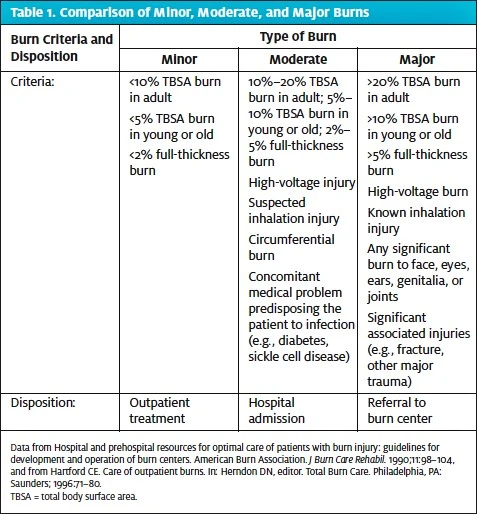
Minor burns include partial-thickness burns of <10% of total body surface area (TBSA) in patients aged 10 to 50 years, partial-thickness burns of <5% of TBSA in patients aged <10 years or >50 years, and full-thickness burns of <2% of TBSA in any patient without other injury. Additionally, to be classified as minor, these burns must be the sole injury and should not include the face, hands, perineum, or feet. Minor burns must not cross major joints or be circumferential. If a burn does not meet those criteria, then it is classified as either a moderate or major burn. Patients with major (severe) burns should be referred to a burn center.3 The criteria for classification and disposition of minor, moderate, and major burns are shown in Table 1.
Discussion
Key Historical Factors
Historical factors play a key role in determining injury type and treatment. The patient, witnesses, family, and emergency medical responders can provide important historical information. The medical history should focus on exposure or cause, duration of substance exposure, estimated temperature of substance(s), comorbid medical illnesses, tetanus status, and other injuries in addition to the burn.2 A concise method of efficient history-taking is the AMPLE method: allergies, medications, past medical history, last meal, events.
Several risk factors impact the prognosis and severity of burns. One retrospective review identified three risk factors associated with a higher degree of mortality: age (>60 years), nonsuperficial burns covering ≥40% of TBSA, and burns associated with inhalational injury.6 Age of the patient is an important factor in the classification of burns and the subsequent morbidity and mortality. The most vulnerable ages for burns are <5 years and >60 years. Abuse must always be considered in children with burns. Burns account for approximately 10% of cases of child abuse.7 For adults, socioeconomic factors that increase the risk of sustaining a burn include nonwhite ethnicity, low household income, crowded household living conditions, low maternal education, and unemployment.8 In all groups, burns are more likely to occur during the winter, when heating appliances are more often used for cooking, heating, and lighting.9
Along with risk factors and socioeconomic factors, comorbid illnesses can greatly impact morbidity. A major comorbid illness associated with burns is epilepsy. Seizures are an important
factor in 29% to 44% of burns.10 Other comorbid illnesses associated with burns include blindness, deafness, arthritis, and diabetes, particularly in elderly patients.11 In addition, patients who have congestive heart failure or renal insufficiency are at higher risk of morbidity and mortality.3,12
Types of Burns
The most common type of burn in children is from a scald injury, although in adults the most common burn occurs from a flame injury. The various types of burns include thermal, cold exposure, chemical burns, electrical current, inhalation, and radiation. The most common
type is thermal, and the depth of the burn injury is related to the temperature of the flame or heated object, duration of contact of the skin with the heat source, and the thickness of the skin. The depth of the burn is the major determining factor in healing. Chemical burns can occur from either acid or alkaline substances. These chemicals can alter pH, disrupt cellular membranes, and lead to toxic effects on various metabolic processes. In electrical burn injuries, the degree of injury depends on the pathway of the current, the resistance to current flow through the tissues, and the strength and duration of the current flow. All high- voltage injuries (>1000 V) are considered severe burns and should be treated at a burn center. Radiation burns most commonly result from prolonged sun exposure in fair-skinned individuals. Although burns from sun exposure are often superficial, the more concerning feature is the ability of ionizing radiation to damage DNA. Inhalational injury is a dangerous complication and commonly results from steam or fire flash burns. Inhalational injuries are also associated with carbon monoxide (CO) poisoning, which result in variable complaints. Loss of consciousness, headache, nausea, vomiting, and dizziness are all common in CO poisoning. Any concern for inhalational injury or CO intoxication warrants emergency medical care and transfer via emergency medical services.
Examination of the Burned Individual
Thorough examination is paramount. Direct assessment of the airway is critical and must include evaluation for injury to the face and neck. Injury to the face, neck, or airway can result in edema, potentially leading to airway compromise. Concern for airway involvement, inhalational injury, or CO poisoning warrants administration of supplemental oxygen and transfer to an emergency department. A careful physical examination from head to toe is the next step. Clothing and jewelry should be removed from involved areas. Areas that are vital to examine in patients with burns include the face, hands, feet, genitalia, perineum, and major joints, because the condition of these is a criterion for transfer to a burn center.2,3,12
Estimating Total Surface Area and Use of Burn Charts
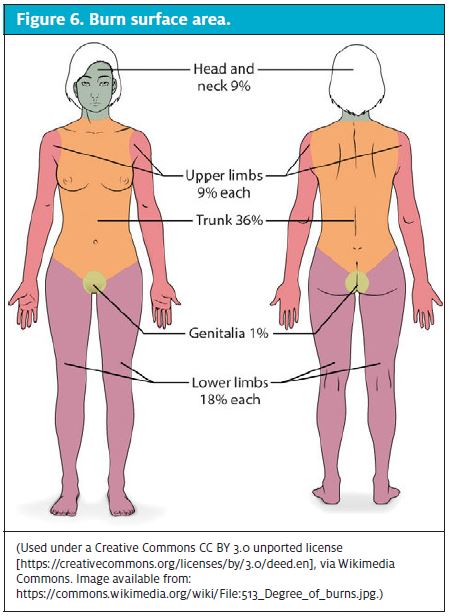
Burn size estimation guides treatment and determines the need for transfer to a burn unit. The extent of a burn is expressed as a percentage of the TBSA, which does not include superficial burns. The two most commonly used methods of determining TBSA in adults are the Lund-Browder chart and the Rule of Nines. The Lund-Browder chart is the most accurate method for determining TBSA in children and adults.13 The Rule of Nines is the most efficient method in adults. In the Rule of Nines, each leg of the patient represents 18% of TBSA; each arm, 9% of TBSA; the anterior and posterior trunk, each 18% of TBSA; and the head, 9% of TBSA (Figure 6). The palm method may be more useful in burns that are irregular. With that method, the palm of the patient’s hand (excluding the fingers) is 0.5% of TBSA. The entire palmar surface, including fingers, is 1% in children and adults.3
High-Risk Burns
High-risk burns are those that require burn specialist assessment and treatment. A burn injury is high risk and requires transfer of the patient to a burn center if it is associated with any of the following12:
- Extremes of age (<5 years or >60 years)
- Burns to the face, hands, perineum, feet, or major joints (partial or full thickness)
- Burns in areas of flexure (such as neck or axilla)
- Circumferential partial or full-thickness burns to the limbs, torso, or neck
- Chemical burn of >5% of TBSA
- Exposure to ionizing radiation
- High-pressure steam injury (because of risk of inhalational injury)
- High-voltage (>1000 V) electrical injury
- Hydrofluoric acid burn >1% TBSA
- Suspicion of nonaccidental injury
- Partial-thickness or full-thickness burns of >5% of TBSA in children and of >10% of TBSA in adults
- Patients with coexisting medical conditions, including a history of cardiac issues (congestive heart failure atrial fibrillation, etc.), immuno-suppression, current pregnancy, and renal insufficiency
Many of these high-risk burns are also included in the Burn Center Referral Criteria described by the Committee on Trauma of the American College of Surgeons14:
- Partial-thickness burns of >10% of TBSA
- Burns involving the face, hands, feet, genitalia, perineum, or major joints
- Third-degree burns (in patients of any age)
- High-voltage electrical burns
- Chemical burns
- Inhalational injury
- Burn patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality
- Any patient with burns and concomitant trauma (e.g., fractures) in which the burn injury poses the greater risk of morbidity and mortality. If the trauma presents the greater risk, then the patient can first be stabilized in a trauma center before transfer to a burn unit.
- Special requirements, such as social, emotional, or long-term rehabilitation needs
- Children who require qualified pediatric personnel and equipment
Main Treatment Options
The initial treatment of minor thermal injuries consists of removing debris, cooling, cleansing, and dressing the wound. In addition, pain management and tetanus vaccination are important. Burn wounds can be cooled after any clothing, jewelry, or other debris is removed. The wound areas can be cooled with room temperature or cool tap water, which provides pain relief and limits tissue injury. One effective method of cooling is applying sterile saline-soaked gauze, cooled to around 50° to 60°F. Direct application of ice should be avoided, which leads to increased damage and pain. To clean burn wounds, a number of burn centers suggest washing minor burns with only soap and water and discourage the use of skin disinfectants, which inhibit the healing process.12,13,15
Debridement includes the cleaning of sloughed or necrotic skin, including ruptured blisters. Extensive debridement can be deferred until the initial follow-up visit. The management of intact blisters is controversial. Blisters that last for several weeks without resorption indicate a possible underlying deep partial-thickness or full- thickness burn, for which the patient should be referred to a burn center.3,12,13
Patients with superficial burns must keep the wound clean and apply nonperfumed moisturizer. These patients do not require topical antibiotic ointment.12,13,15
Patients with partial-thickness burns should be treated with topical antimicrobials, because burn wound surfaces are prone to rapid bacterial colonization. Topical antimicrobial agents and cytoprotective dressings are the best choices for wound coverage; however, there is no consensus on which topical agent or dressing is most effective for burn management. Commonly used topical agents for partial-thickness burns include silver sulfadiazine (SSD), combination antibiotics, mafenide, chlorhexidine, povidone-iodine, bismuth-based gauze, and Dakin’s solution.13,15,16 Of these, SSD is one of the most commonly used topical agents in treating partial thickness burns; it is applied one to two times per day. Historically, it was thought to function by decreasing bacterial colonization of the wound, but there are no well-designed trials that demonstrate improvement in wound healing or reduction of infection, and it has multiple adverse effects.16,17 SSD creates a pseudo-eschar around the wound, which allows microbial colonization around the outer edges. SSD cannot be used in children younger than 2 months or in women who are pregnant or breastfeeding. Its use should also be avoided on the face and around the eyes, because it can cause significant ocular toxicity and scarring. A 2008 Cochrane Review demonstrated that SSD delays wound healing time and increases the need for dressing changes, and the authors provided evidence for other treatment options.16
Other Treatments
- Combination antibiotics: Polysporin contains bacitracin and polymyxin B, usually used for superficial burns involving the face and perineum. Polysporin is nontoxic and does not harm forming tissue. However, it is not effective for methicillin-resistant Staphylococcus aureus or deeper wounds.15,16,18,19
- Mafenide: This functions as a carbonic anhydrase inhibitor and is applied once or twice per day as a cream. It does present a low risk of rash and pruritus and is effective in treating infections.16,18 However, a common adverse effect is metabolic acidosis.
- Chlorhexidine: This is often used in combination with a gauze dressing, and it does not interfere with wound reepithelialization. It is also long-acting.13,16
- Povidone-iodine: This combines broad-spectrum antibacterial activity with a moist environment via its liposomal preparation. However, it is cytotoxic and delays wound healing. It should be applied four times daily.16,19
- Bismuth-based gauze: This is often preferred for clean partial-thickness wounds and can prevent wound infection. It is inexpensive and relatively safe for wound care.16
- Dakin’s solution: This is a broad-spectrum antimicrobial that does eliminate methicillin-resistant S. aureus. It is inexpensive and cytoprotective but can cause pain.13,15,16
Partial-thickness and full-thickness burns generally require dressing, but superficial burns do not. The dressings protect the wound from further trauma or infection, provide comfort and pain relief, and promote healing. Wounds are generally cleansed and dressed daily. There are four major types of dressing used in managing burns3,16:
- Compresses
- Biosynthetics
- Biologics
- Barrier dressings
During the healing process, pruritus is a common problem, but it generally diminishes and then stops after the wound is completely healed. Systemic antihistamines are the first-line therapy. A number of other topical agents, including bicarbonate of soda baths and moisturizing lotions, can also be used.3,16,20
Tetanus immunization should be updated for every burn patient. Tetanus immunoglobulin should be given to patients who have not received a complete primary immunization.3
Pain management is also an important part of treating burn patients. For smaller or less severe burn injuries, pain can be managed with acetaminophen and nonsteroidal anti-inflammatory drugs. Pain generally diminishes greatly once wound epithelialization has occurred. Many options exist for patients with larger or with moderate to severe injuries, and opioids such as morphine are often necessary for pain management.21 [Editor’s note: See the abstract “Patients Should Be Told About Potential Constipation with Opioids” in this issue’s Abstracts in
Urgent Care section.]
Follow-Up Care
Follow-up care in burn patients is important because signs of infection, scarring, and contracture are potential complications of any burn injury. Any patient, either at initial or follow-up presentation, with an infected wound should be hospitalized to minimize the risk of sepsis. For minor burns, follow-up can be done on a weekly basis with the primary physician until wound epithelialization occurs. More frequent follow-up is necessary if there is insufficient pain control, if the family cannot provide adequate care, or if the patient has a biologic or synthetic dressing. After epithelialization of the wound, follow-up visits can be scheduled every 4 to 6 weeks to evaluate for any evidence of hypertrophic scar or keloid formation. If wound epithelialization has not begun after 2 weeks or if follow-up visits show a full thickness burn of >2 cm, patients should be referred to a surgeon with experience in burn care.12,13
Case Resolution
The 62-year-old woman whose case was mentioned at the start of this article has circumferential bilateral forearm burns with blisters, comprising approximately 5% of TBSA. Her jewelry was removed from her upper extremities, and gauze soaked in room-temperature water was placed over the wounds. With her history of diabetes and congestive heart failure, in addition to the circumferential burns, she met criteria for evaluation by a burn center specialist and was referred to one.
Conclusions
The majority of burns seen in urgent care centers are minor and can be treated on an outpatient basis. Minor burns include
- Partial-thickness burns of <10% of TBSA in patients 10 to 50 years old
- Partial-thickness burns of <5% of TBSA in patients <10 years or >50 years old
- Full-thickness burns of <2% of TBSA in any patient without other injury
Burns for which the patient should be referred to a specialist include
- Partial-thickness burns of >10% of TBSA
- Burns involving the face, hands, feet, genitalia, perineum, or major joints
- Full-thickness burns
- High-voltage electrical burns; chemical burns
- Suspected inhalational injury
In addition, a physician must demonstrate sound clinical judgment in determining whether a patient should be referred to a burn center. Treatment of burn patients primarily involves initial cooling, cleansing, and debridement. Multiple regimens exist for outpatient treatment.
References
- Brigham PA, McLoughlin E. Burn incidence and medical care use in the United States: estimates, trends, and data sources. J Burn Care Rehabil. 1996;17:95–107.
- Landry A, Geduld H, Koyfman A, Foran M. An overview of acute burn management in the Emergency Centre. African Journal of Emergency Medicine. 2013;3:22–29.
- Gibran NS; Committee on Organization and Delivery of Burn Care, American Burn Association. Practice guidelines for burn care, 2006. J Burn Care Res. 2006;27:437–438.
- Hospital and prehospital resources for optimal care of patients with burn injury: guidelines for development and operation of burn centers. American Burn Association. J Burn Care Rehabil. 1990;11:98–104.
- Hartford CE. Care of outpatient burns. In: Herndon DN, editor. Total Burn Care. Philadelphia, PA: Saunders; 1996:71–80.
- Ryan CM, Schoenfeld DA, Thorpe WP, et al. Objective estimates of the probability of death from burn injuries. N Engl J Med. 1998;338:362–366.
- Pressel DM. Evaluation of physical abuse in children. Am Fam Physician. 2000;61:3057–3064.
- Edelman LS. Social and economic factors associated with the risk of burn injury. Burns. 2007;33:958–965.
- Peck MD, Kruger GE, van der Merwe AE, et al. Burns and fires from non-electric domestic appliances in low and middle income countries. Part I. The scope of the problem. Burns. 2008;34:303–311.
- Courtright P, Haile D, Kohls E. The epidemiology of burns in rural Ethiopia. J Epidemiol Community Health. 1993;47:19–22.
- Ryan CM, Thorpe W, Mullin P, et al. A persistent fire hazard for older adults: cooking-related clothing ignition. J Am Geriatr Soc. 1997;45:1283–1285.
- Hettiaratchy S, Papini R. Initial management of a major burn: II—assessment and resuscitation. BMJ. 2004;329:101–103.
- Mertens DM, Jenkins ME, Warden GD. Outpatient burn management. Nurs Clin North Am. 1997; 32:343–364.
- Committee on Trauma. In: Chicago, IL: American College of Surgeons: Resources for Optimal Care of the Injured Patient. 6th edition. Guidelines for trauma centers caring for burn patients. 2014:101. Available from: https://www.facs.org/~/media/files/quality%20programs/trauma/vrc%20resources/resources%20for%20optimal%20care%202014%20v11.ashx
- Waitzman AA, Neligan PC. How to manage burns in primary care. Can Fam Physician. 1993;39:2394–2400.
- Wasiak J, Cleland H, Campbell F, Spinks A. Dressings for superficial and partial thickness burns. Cochrane Database Syst Rev. 2013;3:CD002106.
- Hussain S, Ferguson C. Best evidence topic report. Silver sulfadiazine cream in burns. Emerg Med J. 2006;23:929–932.
- Kucan JO, Smoot EC. Five percent mafenide acetate solution in the treatment of thermal injuries. J Burn Care Rehabil. 1993;14(2 Part 1):158–163.
- Norman D. The use of povidone-iodine in superficial partial-thickness burns. Br J Nurs 2003;12(suppl):S30–S36.
- Goutos I, Dziewulski P, Richardson PM. Pruritus in burns: review article. J Burn Care Res. 2009;30:221–228.
21. Patterson DR, Hofland HW, Espey K, Sharar S; Nursing Committee of the International Society for Burn Injuries. Pain management. Burns. 2004;30:A10–A15