Published on
Urgent message: Metacarpophalangeal dislocations involving digits other than the thumb or index finger may be somewhat atypical, but are known to occur as a result of a fall on an outstretched hand—a common precedent to an urgent care visit. Familiarity with management of such injuries precludes the need to refer the patient.
Leonard A. Powell, DO, MS, FACOFP, CMD and Chad E. Richmond, DO
ABSTRACT
Metacarpophalangeal (MCP) joint dislocations typically occur in a dorsal fashion following trauma, most commonly a fall causing hyperextension of the joint. Hyperextension of the MCP joint may lead to avulsion of the volar plate from the metacarpal head or neck. Additionally, fractures of the base of the proximal phalanx or metacarpal head are seen in up to half of cases. The index finger is the most involved location of MCP dislocations, followed by the thumb; it is quite uncommon for the third or fourth digits to be involved. This case concerns a 76-year-old man with a dislocation trauma to the third and fourth MCP joints. Successful closed reduction was performed in the urgent care center at the time of initial presentation.
INTRODUCTION
Metacarpophalangeal joint dislocations are typically traumatic injuries following a fall on an outstretched hand due to hyperextension of the affected joint.1 Hyperextension of the MCP joint may sometimes lead to avulsion of the volar plate from the metacarpal neck at the time of dislocation. Fractures of the base of the proximal phalanx or metacarpal head are seen in up to half of cases.2 A careful diagnosis and treatment of affected structures, as well as ruling out surgical emergencies such as compartment syndrome, are essential to restoring prior function of the affected hand.
PATIENT INFORMATION
A 76-year-old male presented to the urgent care clinic 24 hours postinjury for evaluation of pain and swelling in the right hand following a fall on ice outside of his home. He had no history of trauma or injury to the hand prior to the fall. He had no significant or contributory past medical or surgical history, except for unreported age-related osteoarthritis. He takes no medications and denies any significant alcohol, tobacco, or drug use. He lives at home with his wife and is functionally independent of his activities of daily living and instrumental activities of daily living.
CLINICAL FINDINGS
The patient’s vital signs were stable and afebrile. On presentation, he was noted to have significant soft tissue swelling and moderate ecchymosis about the right hand. The swelling was most evident to the dorsum of the right hand, and diffuse. Some of this extended into the fingers throughout.
The patient had full sensation and good capillary refill, but limited range of motion due to the swelling, and dislocations with deformity. He had a mild but obvious deformity to the third and fourth digits of the right hand, as well as a small abrasion. He demonstrated no signs of infection or bacterial cellulitis, despite the delay in initial presentation.
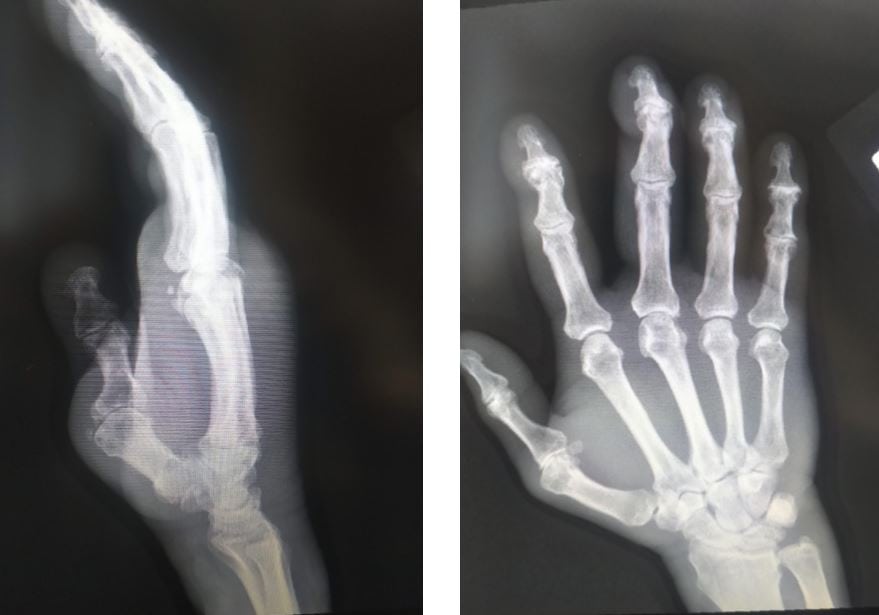
Imaging of the right hand showed extensive soft tissue edema and dislocation of the third and fourth MCP joints with a small avulsion fracture arising from the third metacarpal head. (See Figure 1a and Figure 1b)

The patient’s soft tissue swelling was a slight limiting factor, but edema reduced significantly with reduction alone. The patient’s tendon function was fully intact after reduction, and he was otherwise neurovascularly intact before and after reduction. Postreduction imaging showed proper reduction of the third and fourth MCP joints. See Figure 2a and Figure 2b.
DISCUSSION
Anatomically, the MCP joint is a condyloid joint: the proximal phalanx is composed of a shallow and concave surface with a congruent cam-shaped metacarpal head. Muscular sesamoid attachments are embedded in the volar plate and serve as the point of attachment for muscles such as the adductor pollicis brevis and flexor pollicis brevis muscles. Injury to the MCP can be classified as simple, due to subluxation, or complex, involving interposition of the volar plate and sesamoid bones or metacarpal head entrapment due to displaced natatory ligaments distally or the superficial transverse metacarpal ligament proximally.
Dorsal dislocations may be identified as simple or complex:
- Simple dislocations occur because of hyperextension of the proximal phalanx of the metacarpal head and flexion of the corresponding proximal interphalangeal joint.
- Complex dislocations manifest as bayonet positioning of the proximal phalanx dorsal to the metacarpal shaft and skin dimpling in the proximal palmar crease.
Volar dislocations show extensor lag and dorsal skin depression proximal to the base of the proximal phalanx.
IMAGING
Lateral and oblique views of the hand are best to observe dislocations. Joint space widening can indicate interposition of the volar plate. Entrapment of sesamoid bones in the MCP joint is diagnostic of complex dislocation.
MANAGEMENT
Treatment is dictated based on severity of the dislocation. Closed reduction and immobilization involve applying direct pressure over the dorsal or volar aspect of proximal phalanx. Open reduction involves surgery and should be deferred to orthopedic or hand specialty surgeons. Post-treatment complications that can arise include joint stiffness, post-traumatic arthritis, or osteonecrosis.3
CASE RESOLUTION
The patient underwent closed reduction with a good result of MCP alignment on x-rays. He was also placed in a compression bandage. Volar splinting was avoided due to further fall risk and age-related osteoarthritis comorbidity. He was referred to a hand surgeon for further follow-up and management. He demonstrated no neurovascular compromise either before or after reduction.
CONCLUSION
Metacarpophalangeal joint dislocations occurring in digits other than the index finger or thumb are especially uncommon. Treatment with closed reduction when appropriate and follow-up with orthopedic surgery should be performed.
REFERENCES
- Izadpanah A, Wanzel K. Late presentation of a complete complex thumb metacarpophalangeal joint dislocation: a case report. Plast Surg. 2011;19(4):139–42.
- Wolfe SW, Hotchkiss RN, Pederson WC, et al. Dislocations and ligament injuries of the digits. In: Pederson W, Cohen K, eds. Green’s Operative Hand Surgery. 8th ed. Philadelphia, PA: Elsevier; 2017:278–317.
- An MT, Kelley JP, Fahrenkopf MP, et al. Complex metacarpophalangeal dislocation. Eplasty. 2020;20:ic3.
Author affiliations: Leonard Powell, DO, MS, FACOFP, CMD, Rowan University, Associate Professor of Geriatric Medicine and Osteopathic Manipulative Medicine (OMM). Chad E. Richmond, DO, DAOBFP, Inspira Health physician. The authors have no relevant financial relationships with any commercial interests.

Leonard A. Powell, DO, MS, FACOFP, CMD
