Published on
Francesca Cocchiarale, DO; Alexa Bailey, MS-3; Michael Weinstock, MD
Urgent Message: Pulmonary embolism can be frequently missed as a diagnosis because it can present with a variety of signs and symptoms. Understanding clinical decision rules and myriad presentations can help urgent care providers determine when patients benefit from immediate referral to an emergency department.
Citation: Cocchiarale F, Bailey A, Weinstock M. An Atypical Cause of Fever and Confusion: A Case Report of Delayed Pulmonary Embolism Diagnosis. J Urgent Care Med. 2024; 18(6):28-31
Key Words: pulmonary embolism, fevers, tachycardia, emergency department
Abstract
Introduction: Pulmonary emboli (PE) can manifest with a wide variety of different clinical presentations. This commonly leads to delays in diagnosis.
Clinical Findings: A 63-year-old man with a history of gastroesophageal disease (GERD), hypertension and a recent diagnosis of multiple myeloma who was on lenalidomide presented to the emergency department (ED) with 1 day of fever and confusion. His vitals were remarkable for a temperature of 38.2°C and pulse of 122 beats per minute (BPM). He initially underwent non-contrast computed tomography (CT) of the chest, which showed ground glass opacities in bilateral lungs, suspicious for pneumonia. Toxicology testing was negative. CT angiography of the head and neck also showed no abnormalities to explain the patient’s fever and confusion. The patient was admitted and placed on broad-spectrum intravenous antibiotics.
Diagnosis: After several days of antibiotic treatment, he remained tachycardic and febrile and began to require supplemental oxygen. He also began to complain of left leg pain, which prompted clinicians to obtain bilateral lower extremity venous ultrasound (US). The US showed bilateral deep vein thromboses (DVT) in the posterior tibial veins. After this was discovered, a computed tomography angiography (CT-A) of the chest was ordered, which showed acute bilateral PE, without evidence of right heart strain. The patient was started on rivaroxaban and after receiving 2 doses, his fevers and tachycardia resolved.
Conclusion: It is important to consider a broad list of serious, infectious and non-infectious, diagnoses when patients present with altered mental status and fever.
Introduction
Tachycardia and fever are common symptoms that can be signs of a wide range of pathologies. In the United States, 600,000 of cases of venous thromboembolism (VTE) are diagnosed annually, and PE accounts for more than 100,000 American deaths each year. The 30-day mortality after PE diagnosis approaches 10%.[1] PE can present with a variety of non-specific signs and symptoms, such as tachycardia, elevated temperature, anxiety, syncope, and chest pain.[2] Given the relative frequency, associated mortality, and non-specific presentations for PE, it is important for clinicians assessing undifferentiated patients to include PE on the differential in a variety of presentations.
Case Presentation
A 63-year-old man with a history of gastroesophageal disease (GERD), hypertension, and a recent diagnosis of multiple myeloma presented to the ED with 2 days of fevers at home with a maximum temperature of 38.8°C. He had taken acetaminophen without improvement in his temperature. His wife brought him to the ED because he seemed confused a day after his fevers started. She noted that he was disoriented and did not recognize his family. At the bedside, his wife had to assist him with answering questions. She stated he had not had respiratory symptoms such as cough, rhinorrhea, and shortness of breath. He had not complained of chest pain or headache. He had no history of alcohol, tobacco, or drug use.
Physical and Laboratory Exam Findings
The patient’s vitals in the ED were significant for a temperature of 38.2°C, and a pulse of 122 BPM. His respiratory rate and blood pressure were normal, and the oxygen saturation was 96% on room air. On exam, he appeared ill and anxious and was only oriented to himself. His lungs were clear. He was tachycardic but had a regular rhythm. His abdominal, skin, and extremity exams were unremarkable.
Differential Diagnosis
Many clinical entities were considered in explaining the patient’s presentation of altered mental status, fever, and tachycardia, including encephalitis, meningitis, drug intoxication, alcohol withdrawal, bacteremia/sepsis, brain abscess, urinary tract infection, skin infection, intraabdominal infection, PE, and pneumonia.
Case Timeline and Management
The patient initially presented to the ED given the severity of his symptoms. Labs were obtained including complete blood count, metabolic panel, and hepatic function panel, and all were unremarkable. Urine toxicology screening was negative. Computer tomography of the head and CT angiography study of the head and neck showed no acute intracranial abnormalities. Non-contrast CT of the chest showed ground glass opacities in the lungs, which were believed to represent pneumonia, as well as destructive bone lesions consistent with his known diagnosis of multiple myeloma.
The patient was admitted with a provisional diagnosis of pneumonia and sepsis, and his altered mental status was attributed to delirium from the infection. Due to his immunocompromised status and suspicion of encephalitis, a lumbar puncture was also performed and cerebrospinal fluid analysis revealed no abnormalities to explain his alteration in consciousness. He was started empirically on broad spectrum IV antibiotics.
After several days of receiving antibiotics in the hospital, he remained febrile and tachycardic and began to require supplemental oxygen. He also developed a cough.
On hospital day 6, the patient complained of left leg pain. A lower extremity doppler ultrasound (US) was ordered revealing bilateral DVT in the tibial veins. This subsequently prompted CT-A of the chest, which showed acute bilateral pulmonary emboli.
By hospital day 8, the patient had undergone the following testing:
- Immunocompromised Respiratory Panel: negative for over 20 viral, bacterial, and fungal pathogens
- Echocardiogram: normal ejection fraction and no valvular vegetations
- Bronchoscopy with Bronchoalveolar Lavage: negative for malignant cells or causative organisms
- Blood Cultures: no growth
Diagnostic Assessment and Case Conclusion
The patient was immediately started on rivaroxaban. After receiving just two doses, his fevers and tachycardia resolved completely and he was discharged to follow-up with his oncologist. He was continued on long-term oral anticoagulation and had improvement in his respiratory status.
Discussion
This patient underwent extensive advanced and invasive testing in an inpatient setting for over a week before the ultimate diagnosis of PE was made. Since urgent care (UC) diagnostic resources are dramatically more limited, it’s understandable that the diagnosis of PE would present a challenge for UC clinicians, especially with atypical presentations.
This patient had an unusual presentation for PE. Chest pain, shortness of breath, and cough are the most common symptoms of PE.[3] Although not present in the majority of cases, fever is a relatively common finding present with PE and DVT as well. It is present in up to 33% of patients with VTE within 1 week of diagnosis and has been associated with larger clot burden and higher risk of intensive care unit admission and mortality.[4]
Delirium is an acute and rapidly fluctuating change in cognitive function associated with a trigger, often an acute illness, and is much more common in elderly patients.[5] Unlike fever, delirium is uncommonly caused by PE. Consequently, it’s not surprising that while delirium—which is fully attributable to PE—is a relatively uncommon finding, it has been reported mostly in patients >70 years.[6],[7],[8] Relative to other cases of delirium apparently triggered by PE, the patient presented in this case was somewhat younger.
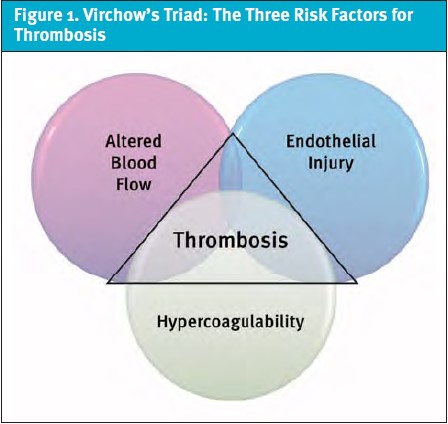
The pathology of VTE involves an understanding of Virchow’s triad (Figure 1). Virchow’s triad consists of hypercoagulability, venous stasis, and vessel wall injury.1 Factors that can also influence development of PE include prolonged immobilization and advanced cancer.[9] The patient in this case had both an advanced cancer diagnosis and prolonged bedrest, for example. However, while the patient’s diagnosis of PE was not confirmed until later in his hospitalization, the resolution of his fever, confusion, and tachycardia after starting anticoagulation lend credence to the idea that the VTE was at least somewhat contributory. It is important to reflect on the components of Virchow’s triad when contemplating VTE as a potential cause of patients’ symptoms.
The patient had persistent tachycardia until his PE was identified and treated. As was the case here, fever in conjunction with tachycardia could prematurely lead clinicians toward anchoring on infectious etiologies. Anchoring bias involves receiving information and relying heavily on the first impression made to guide further decisions made about a situation.[10] UC and ED clinicians are particularly susceptible to anchoring bias since first impressions and initial decisions made in patient evaluation disproportionately affect further care.[11] This is why it is critical to consider PE in the setting of unexplained tachycardia. However, while tachycardia is a common feature in PE, it is only present in ~30% of cases.[12]
The Pulmonary Embolism Rule-Out Criteria (PERC) is a clinical decision rule that is a valuable tool for UC use, as it does not rely on laboratory or imaging. Heart rate is one criterion in the PERC score, and the presence of tachycardia would not allow for PE to be excluded using PERC.[13]
In low-moderate pretest probability situations, d-dimer testing has been found to have a >98% negative predictive value for PE.9 If stat d-dimer testing is available in urgent care, this test could be performed to risk stratify stable patients in whom the PERC rule cannot exclude PE. For patients in whom there is a reasonable suspicion for PE and it cannot be excluded with available clinical decision rules and/or d-dimer testing, immediate ED referral is indicated.
The gold standard diagnostic testing for PE is a contrast-enhanced computed tomography pulmonary angiography (CT-PA).[14] In patients where CT-PA is contraindicated, ventilation/perfusion scanning is an alternative option.14 Initial management of a confirmed PE involves systemic anticoagulation. Direct oral anticoagulation medications such as apixaban, rivaroxaban, edoxaban, and dabigatran are generally preferred for outpatient treatment of VTE due to simplicity of dosing and no requirements for monitoring, as well as generally lower risk of bleeding compared to warfarin.9
Ethics Statement
The patient presented in this case provided verbal consent for the creation of this case study and discussion regarding his care during his inpatient stay. Patient demographics were anonymized in the interest of patient privacy.
Key Takeaways for Urgent Care Providers
- Be aware of tendencies towards anchoring bias and keep a broad differential for undifferentiated patients, especially those with high risk complaints and/or abnormal vital signs.
- Consider the patient’s past medical history thoroughly and what conditions they may be predisposed to, based on their underlying health issues.
- Become familiar with clinical decision rules that can be used with the clinical data available in UC, such as the PERC rule, as these can prevent a number of unnecessary ED referrals when applied correctly.
- Pulmonary embolism can present in a variety of fashions. Consider PE in cases beyond patients with chest pain and shortness of breath.
- Remember not all fevers are due to infection. PE is one example of an important non-infectious cause of fever, and fever occurs relatively commonly in patients with acute VTE.
Author Affiliations: Francesca Cocchiarale, DO, Adena Regional Medical Center. Alexa Bailey, MS-3, University of Kentucky-College of Osteopathic Medicine. Michael Weinstock, MD, Adena Health System, Wexner Medical Center, and The Journal of Urgent Care Medicine. The authors have no relevant financial relationships with any ineligible companies.
Manuscript submitted January 2, 2024; accepted January 30, 2024.
References
- [1]. Turetz M, Sideris AT, Friedman OA, Triphathi N, Horowitz JM. Epidemiology, Pathophysiology, and Natural History of Pulmonary Embolism. Semin Intervent Radiol. 2018 Jun;35(2):92-98. doi: 10.1055/s-0038-1642036. Epub 2018 Jun 4. PMID: 29872243; PMCID: PMC5986574.
- [2]. Ružičić DP, et al. Signs And Symptoms Of Acute Pulmonary Embolism And Their Predictive Value For All-Cause Hospital Death In Respect of Severity of the Disease, Age, Sex And Body Mass Index: Retrospective Analysis of the Regional PE Registry. BMJ Open Respir Res. 2023 Apr;10(1):e001559. doi: 10.1136/bmjresp-2022-001559. PMID: 37076250; PMCID: PMC10124252.
- [3]. Morrone D, Morrone V. Acute Pulmonary Embolism: Focus on the Clinical Picture. Korean Circ J. 2018 May;48(5):365-381. doi: 10.4070/kcj.2017.0314. Erratum in: Korean Circ J. 2018 Jul;48(7):661-663. PMID: 29737640; PMCID: PMC5940642.
- [4]. Saad M, et al. Fever is associated with higher morbidity and clot burden in patients with acute pulmonary embolism. BMJ Open Respiratory Research. Vol. 5,1 e000327. 23 Sep. 2018, doi:10.1136/bmjresp-2018-000327
- [5]. Inouye SK. Delirium in Older Persons. N Engl J Med. 2006;354(11):1157–1165. doi: 10.1056/NEJMra052321.
- [6]. Ahaneku CA, Akpu BB, Njoku CH, Elem DE, Ekeng BE. Pulmonary Embolism Presenting As Delirium: An Acute Confusional State In an Elderly Patient: A Case Report. Egypt J Intern Med. 2023;35(1):8. doi: 10.1186/s43162-023-00193-5. Epub 2023 Feb 6. PMID: 36777903; PMCID: PMC9899661.
- [7]. Carrascosa M, et al. Delirium and Pulmonary Embolism in the Elderly. Mayo Clinic Proceedings. Vol. 84,1 (2009): 91-2. doi:10.4065/84.1.91
- [8]. Jolobe OMP. The spectrum of disturbances in cerebral function in elderly patients with pulmonary embolism. Am J Em Med. 2016;34(3):651. doi:10.1016/j.ajem.2015.12.036
- [9]. Freund, Y., Cohen-Aubart, F., Bloom, B. Acute pulmonary embolism. JAMA, 2022. 328(13), 1336. https://doi.org/10.1001/jama.2022.16815
- [10]. Doherty TS, Carroll AE. AMA J Ethics. 2020;22(9):E773-778. doi: 10.1001/amajethics.2020.773.
- [11]. Ly DP, Shekelle PG, Song Z. Evidence for Anchoring Bias During Physician Decision-Making. JAMA Intern Med. 2023;183(8):818–823. doi:10.1001/jamainternmed.2023.2366
- [12]. Bajaj N, Bozarth AL, Guillot J, KojoKittah J, Appalaneni SR, Cestero C, et al. Clinical features in patients with pulmonary embolism at a community hospital: analysis of 4 years of data. J Thromb Thrombolysis. 2014;37:287–92. doi: 10.1007/s11239-013-0942-8
- [13]. Kline JA, Mitchell AM, Kabrhel C, Richman PB, Courtney DM. Clinical criteria to prevent unnecessary diagnostic testing in emergency department patients with suspected pulmonary embolism. J Thromb Haemost. 2004;2(8):1247-1255. doi:10.1111/j.1538-7836.2004.00790.x
- [14]. Corrigan D, Prucnal C, Kabrhel C. Pulmonary embolism: the diagnosis, risk-stratification, treatment and disposition of emergency department patients. Clin Exp Emerg Med. 2016 Sep 30;3(3):117-125. doi: 10.15441/ceem.16.146. PMID: 27752629; PMCID: PMC5065342.
Click Here to download the article PDF
