Published on
Differential Diagnosis
- Vertebral fracture
- Spondylolisthesis
- Osteolytic lesion
- Abdominal aortic aneurysm
- Lumbar disc herniation
The differential diagnostic considerations for back pain are broad, and are generally divided into mechanical and nonmechanical:
- Mechanical: Lumbosacral strain, herniated nucleus propolsus, epidural compression syndrome, vertebral fracture.
- Nonmechanical: Renal cell carcinoma, pyelonephritis, ureterolithiasis, zoster, retrocecal appendix, abdominal aortic aneurysm.
Diagnosis
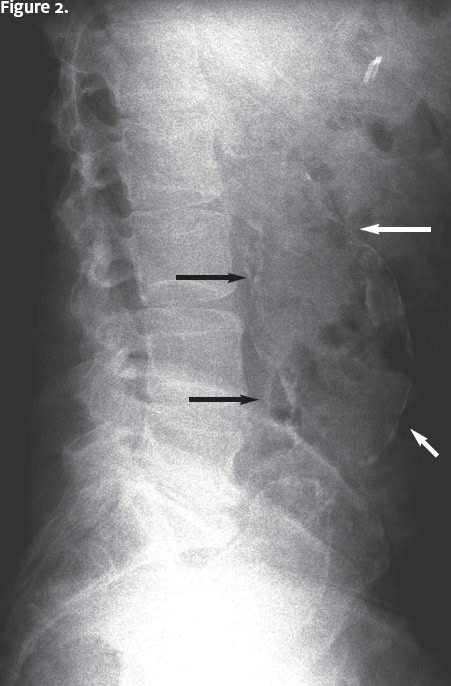
The patient has an abdominal aortic aneurysm (AAA). In the x-ray, curvilinear calcifications are seen anterior to the lumbar spine. These outline the aorta. There is moderate spondylosis at the L5-S1 level, with disc space narrowing. There is no vertebral fracture or focal bone lesion.
Learnings
- AAAs occur most commonly over age 50, in men and in patients with a history of hypertension or smoking.
- AAA is diagnosed as localized enlargement of aorta with a diameter >3 cm, or more than 50% larger than normal diameter.
- There is no role for “therapeutic radiation” with the assessment of nontraumatic back pain.
Pearls for Initial Management and Considerations for Transfer
- The classic “triad” of AAA (abdominal pain, hypotension, and pulsatile abdominal mass) is present less than 50% of the time.
- Surgery is usually recommended with an AAA >5.5 cm in males and >5.0 cm in females.
- Urgent care clinicians should transfer patients with new diagnosis of AAA and back pain, hypotension, tachycardia, or diagnostic uncertainty.
Dull, Constant Back Pain After a Fall: Abdominal Aortic Aneurysm (AAA)
1 2