Published on
Urgent message: The angle of the mandible is one of the most common locations among bilateral mandibular fractures. Bilateral mandibular angle fractures are a rare traumatic event and often occur in the setting of panfacial fractures due to an impacting force.
Chad E. Richmond, DO, DAOBFP; Leonard Powell, DO, MS, FACOFP, CMD; Keith S. Richmond, DMD, MDS.
INTRODUCTION
The mandibular angle is a weak zone that is more exposed to fractures than other areas of the mandibular bone.1 The unbalancing of regional muscles must also be considered as displacement of the fracture often occurs.2 If left untreated, there is often increased morbidity including decreased functional status and decrease in quality of life.
The combined net effects of two temporally separated (by 1 week) bilateral mandibular fractures is presented here.
CASE PRESENTATION
A 24-year-old male presented to an urgent care office with a chief complaint of right-sided jaw pain after a bar fight the previous evening. His history was notable for prior mandibular trauma a week earlier, when he sustained a fracture to the left side of his mandible while playing hockey. His past medical history, past surgical history, and family history were unremarkable. He denies any former or current alcohol, tobacco, or drug use. He reported taking no medications and no allergies to medications. His vital signs were stable and afebrile. He did not experience any bleeding within the mouth during either injury.
CLINICAL FINDINGS
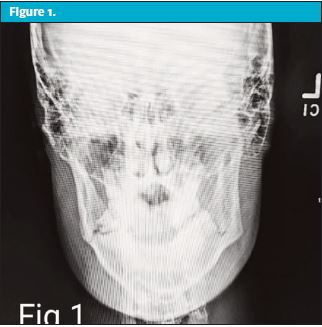
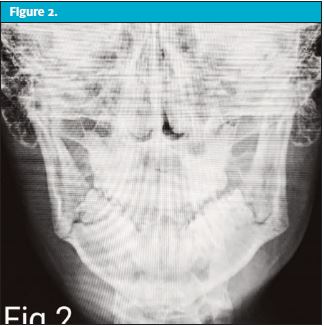
The patient was noted to have right-sided mandibular soft tissue edema, trismus, and residual left-sided mandibular tenderness to palpation, but no problems with speaking, eating, or performing oral hygiene. He did note some discomfort with mastication but did not demonstrate dysphagia. No facial cellulitis was present. There was some slight malocclusion noted upon maximum intercuspation. Imaging of the mandible showed bilateral mandibular angle fractures. (See Figures 1–2 .)
DISCUSSION
A retrospective review of case study presentations reflecting more than 2,000 patients who presented with mandible fractures showed incidence of bilateral presentation simultaneously was only 2.1% over 20 years.2 In all these circumstances, the nature of the fractures was attributable to a single incident.
This patient was being evaluated fairly early for the right fracture but unfortunately not his left. He anecdotally had experienced very few complicating factors up to that point.
If care for these fractures is delayed, however, significant complications can develop.2 These include atrophy of the mandibular muscles; diminished ability for speaking, mastication, and eating; malocclusion; chronic temporomandibular joint pain; facial aesthetic changes; and even “flail mandible” (destabilization of the bony network of the mandible).
All of these sequelae may lead to significant long-term morbidity.
The unbalancing of regional muscles must also be considered as displacement of the fracture often occurs. In bilateral angle fractures, the complexity is manifold because the mandible is split into three fragments: two proximal fragments, the right and left angles influenced by the pterygomasseteric sling, and the temporalis producing a superior vector. The intermediate segment of the distal corpus is acted upon by the mylohyoid and suprahyoid muscles produce an inferior vector.2
The dynamic environment predisposes the angle to high incidence of nonunion or malunion in the event of inadequate reduction and suboptimal fixation.
Ultimately, surgical treatment is required for proper alignment of the fractured segments with fixation of the mandible to stabilize significant opposing forces of a mandible fractured in the three different segments identified previously.
CASE RESOLUTION
Due to the nature of this patient’s injuries, the decision was made to place him on empiric oral antibiotics. He was referred for outpatient dentist evaluation, including consideration for fixation with stable occlusion.
CONCLUSION
Bilateral mandibular fractures are very rare traumatic events, especially when the fractures occur at two different times (as with this patient. Definitive treatment involves surgical fixation to prevent dysfunction involving chewing, eating, and speaking. Dental referral and close follow-up are necessary.
REFERENCES
- Boffano P, Roccia F. Bilateral mandibular angle fractures: clinical considerations. J Craniofac Surg. 2010;21(2):328-331.
- Elavenil P, Mohanavalli S, Sasikala B, et al. Isolated bilateral mandibular angle fractures: an extensive literature review of the rare clinical phenomenon with presentation of a classical clinical model. Craniomaxillofac Trauma Reconstru. 2015;8(2):153-158.
Read Similar JUCM Articles