Published on
Differential Diagnosis
- Sinus tachycardia
- AV nodal reentrant tachycardia (AVNRT)
- AV reentrant tachycardia (AVRT)
- Atrial tachycardia
- Atrial flutter with fixed conduction block
Diagnosis
This patient was diagnosed with atrial flutter, 2:1 conduction. The ECG illustrates a regular, narrow-complex tachycardia at a rate of 150 bpm. There are P waves preceding every QRS complex, most clearly identified in the anterior precordial leads (V1-V3). The intervals are normal and there are no obvious signs of ischemia. There are occasional premature ventricular contractions.
Following identification of a narrow-complex tachycardia and a determination of clinical stability (absence of hypotension or signs/symptoms suggestive of poor perfusion), a detailed evaluation of the ECG can narrow the differential.
First, a regular rhythm as seen in our patient can quickly exclude atrial fibrillation, multifocal atrial tachycardia, and atrial flutter with variable conduction block.
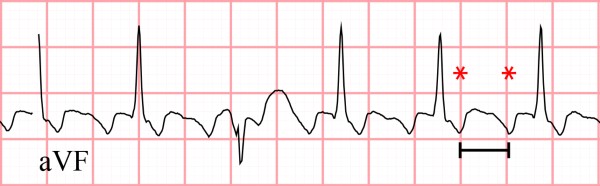
Next, proceed with a careful inspection for the presence of P waves and, if identified, the atrial rate. Accelerated atrial rates (>250 bpm) are associated with atrial flutter or atrial tachycardia. For our patient, we noted initially that P waves were visible preceding every QRS complex in V1-V3; however, there is an atypical appearance to P waves in the limb leads (specifically II, III and aVF) where the expected isoelectric baseline is replaced by identical-appearing “sawtooth” waves (Figure 2). These atrial flutter waves occur at a rate of approximately 300 bpm, complemented by a ventricular rate of 150 bpm, suggesting 2:1 AV conduction.
The morphology of the P wave can offer additional information regarding the origin of tachycardia. P waves suspected to arise from the sinus node are suggested by sharing a similar morphology to a historical ECG in sinus rhythm when available, or having a normal axis (upright in lateral, inferior leads, inverted in aVR). In these cases, sinus tachycardia (appropriate or otherwise), atrial tachycardia, or sinoatrial nodal reentrant tachycardia (SANRT) should be suspected.
The same evaluation of P wave morphology may identify retrograde P waves, where atrial activity originates at the AV node and proceeds backwards (inferior-to-superior), producing inverted P waves in inferior leads. Narrow-complex tachycardias originating at the AV node (producing retrograde P waves) include AVRT and AVNRT.
If P waves are difficult to identify, vagal maneuvers (eg, Valsalva, carotid sinus massage) or adenosine administration and resultant slowing of SA nodal activity and delayed AV nodal conduction may help unmask atrial activity, terminate the arrhythmia, or otherwise offer diagnostic clarity (eg, temporary slowing of sinus tachycardia).
Learnings/What to Look for
- For stable patients with narrow complex tachycardia, begin by determining if the rhythm is regular or irregular. The latter suggests atrial fibrillation, multifocal atrial tachycardia, or atrial flutter with variable conduction block
- When P waves are identifiable:
- Atrial rates greater than 250 bpm suggest atrial flutter or atrial tachycardia
- Look for retrograde P waves; these indicate AVRT or AVNRT
- If P waves are not identifiable, vagal maneuvers or adenosine can aid with diagnosis or terminate certain tachyarrhythmias
Pearls for Initial Management and Considerations for Transfer
- Assess for stability; hypotension or signs/symptoms suggestive of poor perfusion (eg, altered mental status, dyspnea, chest pain) require stabilization and transfer
Resources
- Link MS. Clinical practice. Evaluation and initial treatment of supraventricular tachycardia. N Engl J Med. 2012;367(15):1438-1448.
- Shah RL, Badhwar N. Approach to narrow complex tachycardia: non-invasive guide to interpretation and management. Heart. 2020;106(10):772-783.
- Kumar R, Gupta A, Isser HS. Narrow complex tachycardias-therapeutic and diagnostic role of adenosine. JAMA Intern Med. 2022;182(4):436-437.
Read Similar Articles
- A 96-Year-Old Male With Palpitations And A History Of CAD
- A 46-Year-Old Male Who Presents Due To His Defibrillator Firing