Published on
KEY QUESTIONS
- What features differentiate acute pericarditis from ST-elevation myocardial infarction?
- What are the criteria for diagnosing acute pericarditis?
- What are the treatment options?
What features differentiate acute pericarditis from ST-elevation myocardial infarction?
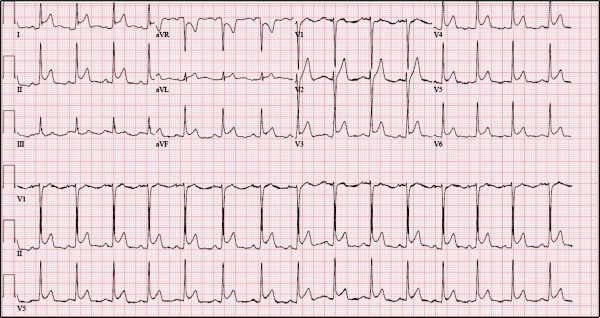
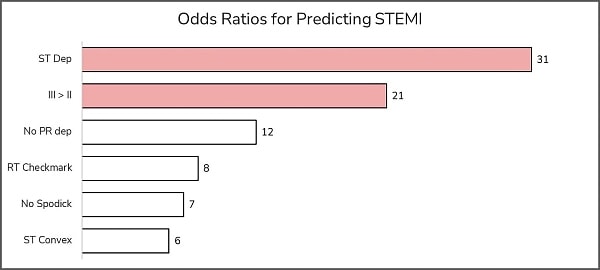
Differentiating pericarditis from ST-elevation myocardial infarction (STEMI) can be challenging. However, features that suggest pericarditis over STEMI include any of the following: diffuse concave-up ST elevations without reciprocal changes; PR depression; PR elevation in aVR; ST-elevation in lead II greater than lead III; and Spodick’s sign—down-sloping of the TP segment. It is important to note that the test characteristics of any single electrocardiographic feature are insufficient to rule in/out pericarditis, and that the feature with the highest odds ratio for predicting STEMI is reciprocal ST-depressions (Figure 1).
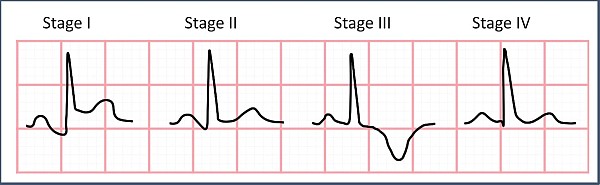
The first 2 weeks are characterized by the above findings. Over several weeks, the ST elevation resolves and the T waves flatten. Next, the T waves invert. Finally, over several weeks, the ECG returns to the patient’s baseline (Figure 2).
What are the criteria for diagnosing acute pericarditis?
The diagnosis is made by meeting two of four criteria:2,3
- Typical symptoms (pleuritic sharp chest pain better when leaning forward)
- New pericardial effusion
- Presence of friction rub
- Typical ECG findings
What are the treatment options?
Colchicine for 3 months and NSAIDs/aspirin tapered over 3-4 weeks are first-line in patients without contraindications.4 It’s reasonable to prescribe a proton pump inhibitor, also. Corticosteroids are reserved for patients with colchicine/NSAID/aspirin contraindication and are not preferred as they are associated with increased recurrence.3
Pearls for Urgent Care Management
- Electrocardiographic features of acute pericarditis include diffuse concave-up ST elevations without reciprocal changes, PR depression, PR elevation in aVR, ST-elevation in lead II greater than lead III, and Spodick’s sign—down-sloping of the TP segment
- Treatment includes 3 months of colchicine and NSAIDs tapered over 3-4 weeks
- Uncomplicated, stable patients with acute pericarditis do not need to be transferred to a higher level of care and can be managed in the outpatient setting
- If the diagnosis is in question, or there are complicating features (eg, instability), transfer to a higher level of care is appropriate
See the video provided by ECG Stampede for detailed analysis.
References
- Witting MD, Hu KM, Westreich AA, et al. Evaluation of Spodick’s sign and other electrocardiographic findings as indicators of STEMI and pericarditis. J Emerg Med. 2020;58(4):562-569.
- Wagner GS, Strauss DG. Marriott’s Practical Electrocardiography. 12th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2014.
- LeWinter MM. Acute pericarditis. N Engl J Med. 2017;371(25):349-359.
- Imazio M, Brucato A, Cemin R, et al. A randomized trial of colchicine for acute pericarditis. N Engl J Med. 2013;369(16):1522-1528.
Read More on Chest Pain