Published on
Urgent message: There are no standardized guidelines for treating patients with chest pain in an urgent care clinic. Using a chest pain protocol with the Marburg Heart Score in a walk-in clinic can assist providers in assuring an appropriate level of care and support standardization in clinician decision-making for treating low-risk chest pain patients.
Lorilea Johnson and Diane L. Smith
Citation: Johnson L, Smith DL. Implementation of a rapid chest pain protocol in a walk-in clinic. J Urgent Care Med. 2022;16(7):19-23.
ABSTRACT
Background
As the walk-in clinic industry has boomed, there are large variances in services provided. There are no guidelines established by regulating bodies to identify criteria for treating patients with chest pain in urgent care clinics.
Purpose
The purposes of this study were to examine the use of the Marburg Heart Score predictive tool in determining the level of risk for patients presenting to a walk-in clinic with chest pain and to quickly identify those at high risk for cardiovascular events.
Methods
A cross-sectional study was conducted in a rural walk-in clinic. Inclusion criteria consisted of persons aged 18 or older who presented to the clinic with complaints of chest pain. Patients with chest pain were identified by front desk staff who initiated chest pain protocols and algorithms. Patient follow-up occurred at 30 and 60 days.
Results
Of the 26 participants, 14 thought their pain might be cardiac. Eight participants met criteria for electrocardiogram and four showed ECG changes. All four participants with ECG changes were sent to the emergency department. The remaining 22 patients were appropriately retained in the clinic where they were assessed, diagnosed, and treated for noncardiac related diagnosis.
Conclusion
The implementation of a rapid chest pain protocol at this walk-in clinic was successful in this study. There was a 100% negative predictive value for cardiac origin of chest pain that was safely retained and treated in clinic. This study provides evidence to standardize clinician decision-making in treating low-risk chest pain patients in an urgent care clinic.
INTRODUCTION
Because of the variability in services from walk-in clinics to urgent care clinics, it has been difficult to standardize protocols in the industry. Medical staff must be able to identify patients with serious conditions and determine if they need to be transferred to receive the appropriate level of care. It is also important to recognize that low-risk patients should be retained for treatment in the walk-in clinic for affordability and convenience of care. There is a need for clarification of the management of patients with chest pain that present at urgent care clinics. Providers within the same clinic may approach chest pain differently, which can be confusing to other staff members. Additionally, chest pain may often be deferred at the front desk with the thought that chest pain needs to be treated in the ED; thus, the patient is never evaluated by a provider at the clinic.
A chief complaint of chest pain can be heart-related, making it potentially life-threatening; however, noncardiac causes are often low risk and are appropriate to be managed in the urgent care setting. Examples of noncardiac causes of chest pain include musculoskeletal pain, gastric esophageal reflux, and lung issues such as pleurisy or bronchitis. Data reflects that over 50% of chest pain seen in the emergency room is not cardiac related.1
The aim of this study was to risk-stratify chest pain patients using the Marburg Heart Score (MHS) and quickly identify high-risk patients who need to be triaged to the ED. The MHS was chosen as the clinic does not have the capability of doing a stat troponin level used in the commonly used HEART Score risk-stratification tool. An additional outcome was to standardize evaluation procedures by using the chest pain protocol algorithms developed for staff and providers at the clinic.
BACKGROUND
There are several predictive scoring tools used to evaluate chest pain. A systematic review was done which compared the following predictive tools: Gencer Rule, MHS, INTERCHEST, Griesel’s Rule, and Bruin’s Slot Rule.2 This study concluded that the MHS was the only validated predictive tool that outperformed clinical judgement in patients with chest pain in outpatient settings.
Previous research has been done in this area using the MHS. A retrospective study done by Radecki, et al was performed to look at the efficiency of four urgent care centers in evaluating patients for coronary artery syndrome. Of the 803 patients in their study, 73 (9.1%) were sent to the ED with 10 patients (1.2%) ultimately diagnosed with acute coronary symptoms. The result was that 673 (83.9%) of the patients were safely managed without referral to the ER.3
As previously mentioned, one of the most popular coronary predictive tools is the HEART score. The letters in the acronym stand for history, ECG, age, risk factors, and troponin levels. A study done by Stopyra, et al4 which evaluated the use of the HEART score concluded that it had a 100% negative predictive value for identifying patients without a coronary artery event from index visit through 1 year. Research has shown that emergency departments that risk stratify patients using the HEART score can decrease length of stay by discharging low-risk patients safely with low risk or a cardiac event.5 Patients with low-risk chest pain and negative diagnostic results that are admitted for observation are found to rarely have a cardiac event but are at increased risk of iatrogenic complications.6 As the HEART score requires a troponin level which is not available at the walk-in clinic, an alternative predictive tool was required.
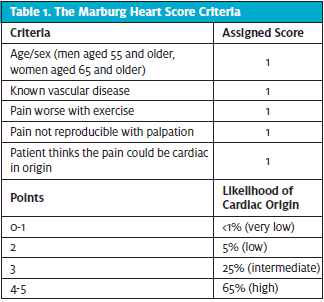
The Marburg Heart Score
The MHS is a predictive tool used to calculate the risk of cardiac event in patients with chest pain. This tool was developed and validated by a German physician, Stefan Bosner, MD, to rule out coronary artery disease in patients with chest pain in primary care clinics without access to troponin levels or ECGs.7 The MHS is a simple five question tool with each question assigned a one-point value (Table 1). Scores of two or less have a negative predictive value of ~98% of a cardiac event and are considered appropriate to treat in outpatient setting. Scores of three and above stratify a higher level of risk but does not rule in coronary heart event and requires additional clinical assessment such as patient examination, vital signs, history, and ECG. In a study of patients in the family practice setting (n=258), the MHS was used to identify patients with acute coronary syndrome (ACS). Used in conjunction with the clinician’s assessment MHS safely reduced emergency department referrals by 19%.8 For these reasons, it was determined that the MHS would be an appropriate tool to include in the rapid chest pain protocol for this study.
METHODS
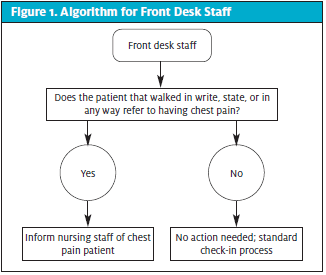
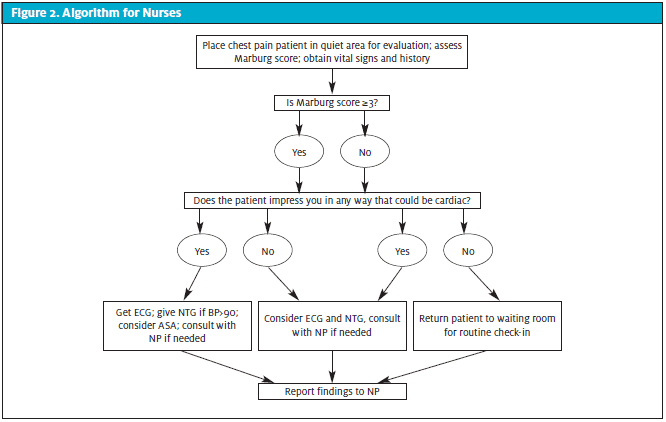
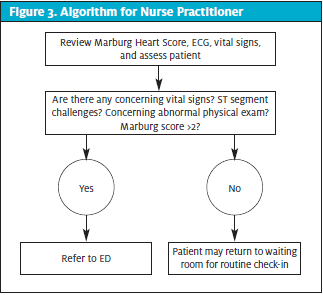
This cross-sectional study was conducted in a walk-in clinic in Southeast Missouri between the dates of November 1, 2020, and January 31, 2021. HIPAA and standard research ethical guidelines were observed in the development, implementation, and analysis of the study. Front desk staff, nurses, and nurse practitioners received training in obtaining informed consent from patients and in the use of the algorithm relevant to their role in the study. Inclusion criteria consisted of persons aged 18 or older who presented to the clinic with complaints of chest discomfort. Patients with chest pain were identified by front desk staff who promptly notified nursing staff for evaluation prior to completing the check in process (Figure 1). The nurses obtained basic history and assessed patients including obtaining vital signs and determining the Marburg Score. An ECG was obtained if the algorithm criteria was met (Figure 2). The provider reviewed the data, evaluated the patient, and determined the disposition of the patient (Figure 3). Patients deemed low risk returned to standard check-in process to be evaluated in clinic. Higher-risk patients as determined by the provider were transferred to emergency department of the affiliated hospital. Phone follow-up and chart review was completed at 30 and 60 days on all 22 low-risk patients to assess their cardiac status and to validate the accuracy of the chest pain protocol.
RESULTS
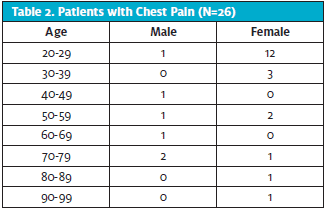
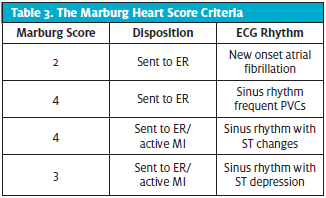
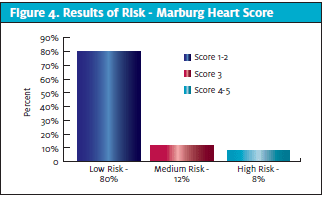
During the three-month period, 26 participants met the criteria for the study. Four participants were male and 22 were female. Participant ages ranged from 22 to 94 with an average age of 38. (See Table 2.) Fourteen participants felt that their chest pain might be heart related. Twelve participants had a score of one point on the MHS, nine participants scored two points, three scored three points, and the remaining two scored four points (Figure 4). Eight out of the total group (n=26) had an ECG performed. Four of these were found to have ECG changes: two had ST segment changes and were diagnosed with myocardial infarction, and two had a new onset of rhythm changes, one with atrial fibrillation and one with supraventricular tachycardia with frequent premature atrial contractions, which were evaluated and treated. All four with ECG changes were sent to the emergency department. (See Table 3.)
The remaining 22 patients were appropriately retained in the clinic where they were assessed, diagnosed, and treated for non cardiac-related diagnosis. Phone follow-up and chart review at 30 and 60 days revealed that none of these patients developed a cardiac related issue in during that time frame.
DISCUSSION
This study addressed the need for criteria which identifies the appropriateness of treatment for patients with chest pain in walk-in clinics and standardization of evaluation of chest pain among providers. The MHS was selected as the predictive tool for this study because it does not require a troponin level like other predictive tools such as the HEART Score or the TIMI Risk Score. The site in which this study was conducted does not have access to rapid troponin levels. Unlike the original studies validating the MHS, this clinic does have access to ECG which was used in the protocol. It is important to note that the MHS is appropriate for urgent care clinics without access to troponin levels or ECG as diagnostic tools. Additionally, algorithms developed for front desk staff and the nurses allowed for standardization of assessment across all disciplines.
Schols (2019) reported that MHS could accurately rule out ACS in the patients estimated to be at low risk.8 In this study, there was 100% appropriate disposition of patients which indicates a 100% negative predictive value for cardiac event in the 22 patients kept and treated in the clinic using this protocol. The potential implications of treating low-risk patients in the urgent care clinic setting rather than sending them to the emergency department include decreased utilization of resources, convenience for the patient, and less potential for over testing and false positive results.9
While the MHS stratifies levels of cardiac risk in chest pain patients, the results never override the clinician’s interpretation of the overall patient presentation but should be considered a tool to help guide the clinician’s decision making. The importance of following the chest pain protocol and established algorithms cannot be underestimated. In this study, one of the four patients sent to the emergency department had a MHS score of two which is categorized as low risk. However, this patient had a new onset of atrial fibrillation discovered on the ECG performed in the walk-in clinic which made emergency department evaluation appropriate. In this specific case, the provider did communicate with the emergency department physician for further direction on patient disposition and care. As well, two patients with MHS scores of three which is classified as medium risk were appropriately kept in the clinic and treated for noncardiac chest pain after further evaluation by the provider. Thus, the additional assessments by the nurse and provider are credited for the appropriate disposition of these patients.
It should be noted that the original validation studies on the MHS included adults ages 35 and older. This study encompassed patients 18 and older; fourteen of the 26 participants were under the age of 35. Younger patients can and do have rhythm changes or palpitations with true supraventricular tachycardia (SVT).
LIMITATIONS
Limitations of this study include a small sample size and single site design. The participants were determined based on presenting compliant of chest pain and this purposive sampling resulted in a population that was disproportionately female (22 female and four male). There was no baseline for comparison as patients are often referred to the emergency department without being checked in when they mention chest pain.
When considering the MHS criteria, clinicians should recognize that patients who have known vascular history and are 55 or older for males, or 65 or older in females, will always start with a score of two. Thus, provider evaluation is essential in scores over three, especially recognizing that other questions have the potential to skew the score higher even when source is noncardiac.
CONCLUSIONS
The implementation of a rapid chest pain protocol was successful in this study and should be continued in the clinic. The algorithms provided consistency in evaluation of patients with a complaint of chest pain. It increased the confidence of providers in assessing heart related chest pain. All patients were correctly directed to appropriate level of care for their condition. This gave a 100% negative predictive value for cardiac origin of chest pain that was safely retained and treated in the outpatient clinic. Evidence was provided to support clinician decision-making in treating low-risk chest pain patients in a walk-in clinic. Implementing this protocol increased the awareness of what can be considered low-risk cardiac pain among clinic providers.
RECOMMENDATIONS
Replication of this study using larger sample sizes and multicenter urgent care clinic locations is recommended. Additionally, further studies in patients below the age of 35 is recommended to validate the findings in this young population and explore the value of using the MHS in this population.
Use of the algorithms for clinic staff could provide consistency in future studies and increase continuity of care in other walk-in clinics. As MHS was initially developed for sites without access to ECG or troponin levels, clinics without these capacities may find the chest pain protocol particularly beneficial. Further research and validation of the chest pain protocol could provide data to address the question of whether all patients presenting to walk-in clinics deserve a basic medical examination and cardiac screening regardless of that clinic’s diagnostic capabilities.
REFERENCES
- Teragawa H, Oshita C, Orita Y. Is noncardiac chest pain truly noncardiac? Clin Med Insights: Cardiol. 2020;14:1179546820918903.
- Harskamp RE, Laeven SC, Himmelreich, JC, et al. Chest pain in general practice: a systematic review of prediction rules. BMJ Open. 2019;9(2):e027081.
- Radecki RP, Foley KF, Elzinga TS, et al. Pilot of urgent care center evaluation for acute coronary syndrome. Am J Manag Care. 2019;25(5):e160-e164.
- Stopyra J, Riley R, Heistand B, et al. The HEART pathway randomized controlled trial one-year outcomes. Acad Emerg Med. 2018;26(1):41-50.
- Finnerty NM, Weinstock MB. Can the HEART score rule out acute coronary syndromes in the emergency department? Ann Emerg Med. 2018;72(6):668-669.
- Weinstock, MB, Weingart S, Orth F, et al. Risk for clinically relevant adverse cardiac events in patients with chest pain at hospital admission. JAMA Intern Med. 2015;175(7):1207-1212.
- Bosner S, Haasenritter J, Becker A, et al. Ruling out coronary artery disease in primary care; development and validation of a simple prediction rule. CMAJ. 2010;182(12):1295-1300.
- Schols AMR, Willemsen RTA, Bonten, TN, et al. A nationwide flash-mob study for suspected acute coronary syndrome. Ann Fam Med, 2018;16(5):296-303.
- Barbarash S, Lebron-Gallagher D, Julson H, et al. A multicenter study of the rate of MACE in chest pain patients with a moderate HEART risk score referred from urgent care for an expedited outpatient cardiology evaluation. J Urgent Care Med. 2020;14(11):31-35.
Author affiliations: Lorilea Johnson, FNP-BC, DNP. Diane Smith, DNP, RN, Missouri State University, School of Nursing. The authors have no relevant financial relationships with any commercial interests.

Lorilea Johnson, FNP, BC, DNP
