Published on
What electrolyte disturbances cause the interval problem seen in this ECG?
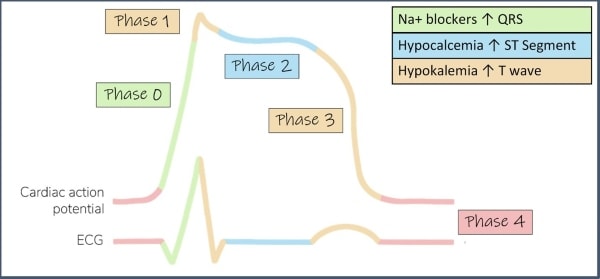
Hypokalemia, hypomagnesemia, and hypocalcemia can all cause a prolongation of the QT interval. While hypokalemia and hypomagnesemia both delay the repolarization phase (phase 3) of the of the cardiac action potential (creating wide-based T waves, U waves, or a fusion of both), hypocalcemia prolongs the QT interval by way of extending the plateau phase (phase 2) of the cardiac action potential (lengthening the ST segment but with a normal T wave, Figure 2). This ECG is consistent with hypokalemia and/or hypomagnesemia.1
Which dysrhythmia is this patient at risk for?
This patient is at risk for torsades de pointes due to early afterdepolarizations/triggered activity during the repolarization phase (R on T phenomenon).2It’s worth noting that the QT correction formulas (eg, Bazett’s formula) are not very good outside a normal heart rate range, and that data supporting the use of a QT nomogram are emerging.3,4 Measuring the QT can be challenging, and many different methods exist. One simple method is the “half the RR” rule—the QT interval is prolonged if it occupies more than half the RR interval. The “half the RR” rule is a conservative estimate at normal and tachycardic rates; perhaps a better option at bradycardic rates is an absolute cut-off of 485 ms.4

See the video provided by ECG Stampede for detailed analysis.
Pearls for Urgent Care Management
- Symptomatic patients with prolonged QT should be transferred to a higher level of care
- Common electrolytes that cause prolonged QT include hypokalemia, hypomagnesemia, and hypocalcemia. If able, commence electrolyte repletion prior to transfer
References
- Diercks DB, Shumaik GM, Harrigan RA, et al. Electrocardiographic manifestations: electrolyte abnormalities. J Emerg Med. 2004;27(2):153-160.
- Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS Guideline for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. J Am Coll Cardiol. 2018;72(14):e91-e220.
- Isbister GK. Risk assessment of drug-induced QT prolongation. Austral Prescrib. 2015;38(1):20-24.
- Rischall ML, Smith SW, Friedman AB. Screening for QT prolongation in the emergency department: is there a better “rule of thumb?” Western J Emerg Med. 2020;226(2).