Published on
Differential diagnosis:
- ST-Elevation myocardial infarction (STEMI)
- Non-ST-elevation myocardial infarction (NSTEMI)
- Hypokalemia
- Long QT Syndrome
- Digoxin toxicity
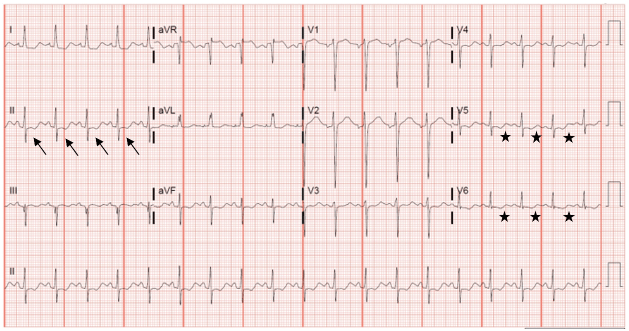
Figure 2. ST depressions are seen in multiple areas of this ECG, illustrated in lead II with arrows. V5 and V6 demonstrate T-wave inversion with prominent U-waves and a long QU interval (stars).
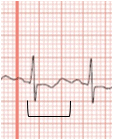
Figure 3. The QU Interval shown here is clearly longer than half of the R-R interval (a simple way to determine if the QT interval is long for the given rate).
Diagnosis
The ECG reveals sinus tachycardia at a rate of 115 beats per minute. The increased amplitude and width of the P wave, ST depression, T wave inversion, and prominent U waves in V5 and V6, and apparent long QT (actually QU interval) all suggest the presence of hypokalemia. Prominent U waves will often give the appearance of a biphasic T wave (“down” then “up,” as opposed to the more ischemic appearing “up” then “down” variety).
A note about tachycardia
Tachycardia is protective in patients with hypokalemia because as the heart rate decreases, the QT interval lengthens. With profound bradycardia and a long QT interval, the heart may depolarize, or ventricular ectopy may occur, while still in the repolarization phase. This “R-on-T phenomenon” (or R-on-U in this case) may induce polymorphic ventricular tachycardia, or torsades de pointes. Since tachycardia is protective for torsades de pointes, one treatment to intentionally accelerate the heart rate is overdrive pacing—which can be performed via pharmacologic means as well as transvenous or transcutaneous pacing. The presence of a malignant dysrhythmia is the only indication for rapid repletion of potassium. If cardiac arrest is imminent or has occurred, administer an initial infusion of 10 mEq IV over 5 minutes and repeat once if needed.
Learnings/What to Look for
- With moderate-severe hypokalemia, look for:
- Increased width and amplitude of the P wave
- Prolonged PR interval
- T-wave flattening or inversion
- ST depression
- Prominent U-waves
- Long QU interval
- In severe hypokalemia, patients develop ectopic beats, supraventricular tachyarrhythmias, and eventually ventricular arrhythmias (particularly torsades de pointes)
Pearls for Urgent Care Management and Considerations for Transfer
- Hypokalemia is often accompanied by hypomagnesemia—don’t forget to check and replace both to decrease the risk of ventricular arrhythmias
- Treatment of hypokalemia involves oral and/or parenteral routes, as well as identification and treatment of the underlying cause of the electrolyte disorder
- In the setting of hypokalemia and a prolonged QT interval (>500 msec), consider transfer to an emergency department or admitting facility where electrolytes can be replaced while the patient is monitored
Resources
- Diercks DB, Shumaik GM, Harrigan RA, et al. Electrocardiographic manifestations: electrolyte abnormalities. J Emerg Med. 2004;27(2):153–160.
- Glancy DL, Wiklow FE, Rochon BJ. Electrocardiogram after 2 weeks of diarrhea. Proc (Bayl Univ Med Cent). 2010;23(2):173–174.
- Levis JT. ECG diagnosis: hypokalemia. Perm J. 2012;16(2):57.
- 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2005;112(24 Suppl):IV1-203.
Acknowledgement: Case presented by Catherine Reynolds, MD, Assistant Professor, Director of Student Clerkships, The University of Texas Health Science Center at Houston.