Published on
Urgent Message: The prediction model developed for this study suggests that tympanometry may have value in evaluating cases of possible acute otitis media or acute hearing loss in urgent care centers.
Jeff Lacour, MD; John Weissert; Dan Frankowski; Demetrio Aguila III, MD; Joshua Russell, MD
Keywords: tympanometry; acute otitis media; otitis media with effusion; sudden sensorineural hearing loss; conductive hearing loss; urgent care
Abstract
Introduction: Tympanometry is a well-validated and rapid tool for assessment of tympanic membrane mobility. Despite American Academy of Pediatrics and American Academy of Otolaryngology guidelines endorsing tympanometry’s value in cases of possible acute otitis media and acute hearing loss, most urgent care (UC) centers do not offer tympanometry. This study used UC data and statistical modeling to predict tympanometry use and its financial implications in UC.
Methods: This was a retrospective cohort study of 140,894 de-identified, real-world UC encounters collected via Intellivisit (IV) software between May 2024–March 2025. A regularized linear regression model was developed to predict encounters in which tympanometry use would be indicated. Two board-certified otolaryngologists independently validated the model’s predictions. Then, the model was used to estimate tympanometry use across 10,000 random, real-world UC encounters. A financial analysis was conducted to estimate the expected revenue associated with tympanometry implementation in UC.
Results: The final model achieved a median F1 score of 0.80 (95% confidence interval [CI] 0.65–0.95) with a sensitivity of 0.55 (95% CI 0.38–0.80), a specificity of 1.00 (95% CI 0.99–1.00), and near-perfect inter-rater agreement between human experts (κ=0.9). Among 10,000 UC encounters, 1,819 (18.2%) were predicted to warrant tympanometry. The financial modeling analysis predicted an average UC center would break-even after 214 tympanometry exams and could generate $4,862 in monthly recurring revenue.
Conclusion: The regression model was able to reasonably identify UC encounters where tympanometry would be clinically indicated. The model suggested that tympanometry would be useful in over 18% of UC cases and, therefore, would quickly be financially viable in an average UC setting. Given the frequency with which ear and hearing complaints were seen among this real-world UC encounter set, tympanometry has the potential to meaningfully affect the quality of care and resource utilization for many UC patients.
Introduction
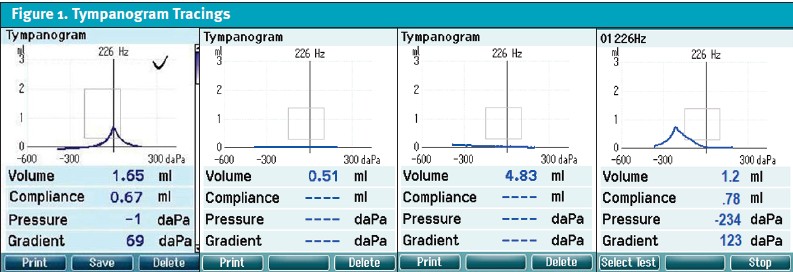
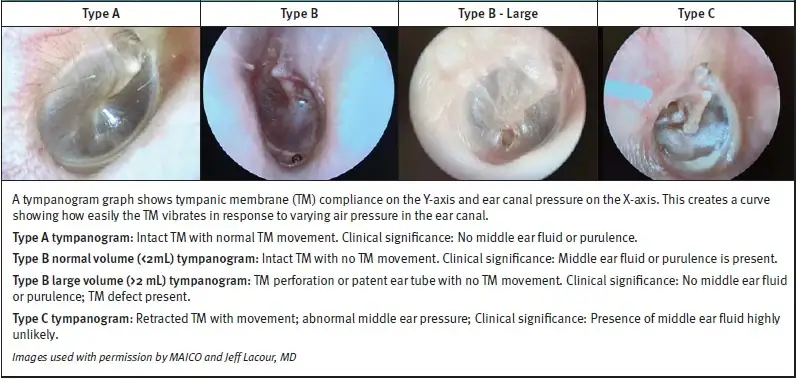
Tympanometry was first introduced in clinical use in the mid-1970s as a novel method to assess movement of the tympanic membrane (TM).[1] Tympanometry involves the use of pressurized air in the external auditory canal (EAC) to assess TM mobility.[2] The device outputs a graphic representation called a tympanogram, which may be one of several types, termed type A, B, or C.[3] A type A tympanogram indicates normal TM movement and absence of a middle ear effusion. A type B (flat) tympanogram indicates no movement of the TM and suggests a middle ear effusion. A type C tympanogram indicates retraction of the TM and negative pressure in the middle ear. A large volume, flat type B tympanogram indicates either a patent ear (P/E) tube or TM perforation (Figure 1).3,[4]
Historically, tympanometry use was limited to otolaryngologists and audiologists; however, advances in technology have made tympanometry accessible to general practitioners. Modern tympanometers are compact, affordable, and require little training to use.[5],[6] Clinicians (ie, physicians, physician assistants, and nurse practitioners) can perform tympanometry themselves or delegate it to medical assistants in most U.S. states.[7] Modern tympanometers are hand-held devices, similar in size to an otoscope, which provides results within seconds, and non-otolaryngologist clinicians can quickly be trained to interpret the results (Figure 2).5,6 Additionally, when used appropriately, tympanometry can be billed separately from evaluation and management (E/M) codes with an average reimbursement of $22–25 United States Dollars (USD) per exam.[8]
Acute otitis media (AOM) is among the most common diagnoses where antibiotics are prescribed in ambulatory settings, particularly in children.[9] In children aged 15-27 months, otalgia accounts for 35.5% of urgent care (UC) and 19.5% of emergency department (ED) encounters.[10] The American Academy of Pediatrics (AAP) guidelines state that AOM cannot be diagnosed without the presence of a middle ear effusion confirmed by assessment of tympanic membrane (TM) mobility with either tympanometry or pneumatic otoscopy.[11] Without adjuncts, the sensitivity of otoscopy for middle ear effusion is as low as 61% with myringosclerosis frequently being mistaken as a middle ear effusion.[12] The addition of tympanometry to otoscopy increases the sensitivity of middle ear effusion detection to greater than 90%–94%. While pneumatic otoscopy has similar sensitivity to tympanometry and slightly better specificity, its use and interpretation require considerable training and experience.12 Despite the above AAP guideline, clinicians rarely assess TM mobility.[13] Reliance on otoscopy alone could explain the high variability in the odds of children being diagnosed with AOM, which has been shown to vary by up to 300% between clinicians seeing similarly matched patients.[14]
Additionally, the American Academy of Otolaryngology (AAO-HNS) guidelines strongly recommend the use of tympanometry when uncertainty exists regarding the presence of otitis media with effusion (OME) in children.4 The justification for this recommendation centers around conductive hearing loss associated with OME (an average deficit of 28 dB) which, if unresolved or untreated (with pressure equalization [PE] tubes) within 3 months, can increase the risk of speech, language, and developmental delay.[15] While no peer reviewed studies to date have been published reporting the prevalence of otalgia, OME, or AOM among children in UC settings, over 90% of children will have OME at some point in the first 2 years of life.[16] Additionally, AOM is diagnosed in nearly one-fourth of children <2 years presenting to the ED with fever.9,[17] Anecdotally, similar trends have been observed by the authors in UC settings. This underscores the imperative for accurate diagnosis of AOM and OME in UC settings, which are often the initial site of care for children suffering from otalgia.
Among adult patients, UC is often the site of initial evaluation for both otalgia and acute hearing loss. Unlike in children, AOM is not a leading cause of otalgia in adults, and more cases are attributable to non-otologic or referred sources.[18] For example, temporomandibular disorder (TMD) is a leading cause of referred otalgia with most patients reporting ear pain and fullness.[19],[20] Frequently, adults with TMD are given an incorrect diagnosis of AOM and antibiotic prescriptions.19 If tympanometry were implemented in such cases, a normal type A tympanogram could exclude middle ear effusion, suggesting a greater probability for non-otologic etiologies, such as TMD.[21]
Acute hearing loss also commonly presents initially to UC and ED settings. Sudden sensorineural hearing loss (SSNHL) is an underrecognized condition and considered an otolaryngologic emergency.[22],[23] Accurate diagnosis of SSNHL is dependent on distinguishing the cause from a conductive hearing loss (CHL) (ie, resulting from OME). The AAO-HNS guidelines advocate for tympanometry to clarify the cause of hearing loss.22 Prompt diagnosis and treatment of SSNHL is correlated with a higher likelihood of return of hearing.23,[24] Many patients will fail to respond to oral steroids adequately and require transtympanic steroid injections (ie, next-line therapy), which are most effective when administered within 1 week of symptom onset.[25] This highlights the urgency of distinguishing between CHL and SSNHL, which, if facilitated by tympanometry, can ensure timely otolaryngology referral.22
Artificial intelligence (AI) algorithms have gained considerable traction in recent years as tools to support evidence-based clinical decisions and to mitigate heterogeneity in clinician practice patterns around common conditions.[26] Given the lack of familiarity that many UC clinicians and staff have with tympanometry, we aimed to determine if a clinical-support machine learning (ML) algorithm could provide guidance for appropriate UC cases in which tympanometry would be likely to aid in diagnosis and management.
Objectives
The primary objective was to determine if a prediction model could be used to identify UC patients for whom tympanometry would be clinically indicated. Secondary objectives included application of the prediction model to estimate the frequency with which tympanometry would be indicated among UC patients and, finally, to assess the financial viability of tympanometry if it were implemented in a hypothetical UC setting using the prediction model.
Methods
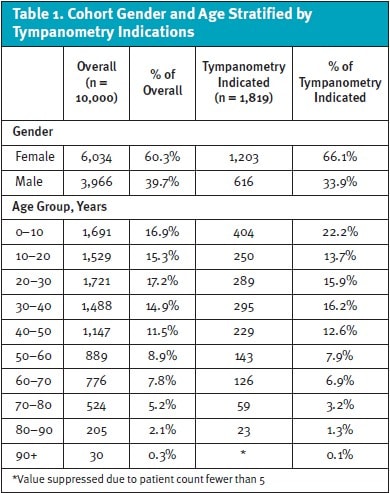
This was a retrospective cohort study of de-identified UC patient encounters (Table 1). Initially, a regularized linear regression model for tympanometry was developed and trained in R-statistical software (R-Project, version 4.4, Vienna, Austria) based on previously described methods,[27] using 140,894 training UC patient encounters. These occurred from May 2024–March 2025 where the presenting symptoms were recorded in Intellivisit (UCP-Merchant Medicine, Minneapolis, MN). Intellivisit (IV) is an algorithmic clinical support software tool designed to enhance efficiency and guideline-adherent care in UC settings. IV collects de-identified data, including demographics, vital signs, chronic conditions, and current symptoms, via a guided interview administered by staff members (eg, medical assistants, nurses) when the patient is roomed.
The initial regression model was developed using a list of target diagnoses (Supplemental Material on jucm.com). This list was developed by using ICD-10 codes that are indicated as appropriate for tympanometry reimbursement by the Centers for Medicare and Medicaid Services (CMS). Once the initial model was developed, it was validated by manual review of 100 cases (50 cases predicted by the model to either use or not use tympanometry) presented in a random order. Manual labeling was performed by 2 board-certified otolaryngologists (JL, DA) to confirm the model’s accuracy based on both clinical expertise and the AAO-HNS guidelines. The 2 reviewers were blinded to their counterpart’s labels. Cohen’s Kappa was used to assess inter-rater agreement. Accuracy was measured using sensitivity, specificity, and F1 with reviewer labels as the reference “gold standard.” We used a bootstrap calculation to estimate the 95% confidence intervals (CI) of F1, specificity, and sensitivity.
To address the secondary objectives, the validated model was then applied to a unique random sampling of 10,000 UC encounters collected with IV to determine the frequency with which tympanometry was predicted to be indicated in a representative UC setting.
Finally, a simple financial analysis was performed to determine the economic feasibility of tympanometry implementation in a UC setting. The cost of a tympanometer was estimated using the price for a device likely to be used in UC centers (MAICO easyTymp, $4,700 USD). The price of which includes training and maintenance for the device.[28] Tympanometry reimbursement was estimated using the low end of average reimbursements reported by CMS,8 which was $22 USD per exam. Tympanometry can be billed in any outpatient setting using the Current Procedural Terminology (CPT) code 92567.8 Annual UC encounter volume was estimated to be 14,750 visits based on Urgent Care Association benchmarking data.[29]
Ethics Statement
Given the use of only de-identified cases without protected health information, this study was exempt from Institutional Review Board evaluation as it did not meet criteria for human subjects research. There was no outside funding for this study, and authors and labelers were uncompensated for their contributions.
Results
To address the primary objective, we found that the prediction model achieved a median F1 score of 0.80 (95% CI 0.65–0.95). The model has a median sensitivity of 0.55 (95% CI 0.38–0.80) and specificity of 1.00 (95% CI 0.99–1.00), indicating probable clinical utility to predict encounters which likely benefit from the use of tympanometry. The validity of expert labels as the “gold standard” was confirmed by the high rate of agreement between the otolaryngologist reviewers (κ=0.9).
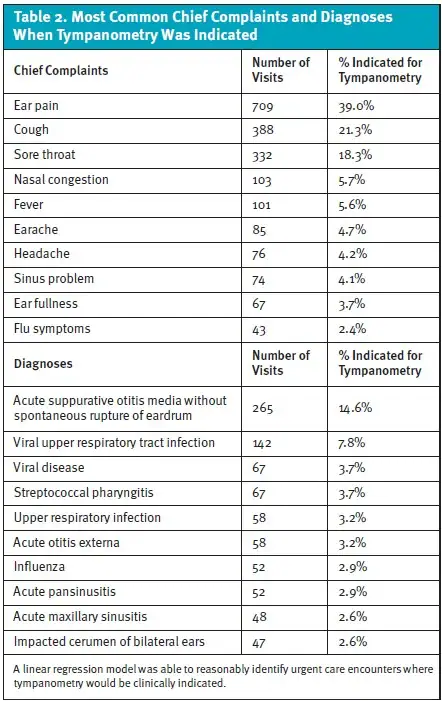
For the secondary objective, we found that, among the random sample of encounters to which the model was applied, 1,819/10,000 (18.2%) were predicted as having an indication for tympanometry. The most common chief complaint and UC diagnosis for encounters where tympanometry was predicted were ear pain and AOM, respectively (Table 2).
Financial Modeling
Assuming $22 reimbursement per tympanometry exam and a one-time device cost of $4,700, UC centers could be expected to reach a “break-even” point after 214 tympanograms. If 18.2% of all UC patients were candidates for tympanometry, this would translate to 2,657 exams annually per center assuming the national average of 14,750 visits per center per year.29 If these exams were distributed evenly month-over-month, 221 tympanometry exams would be performed monthly. Based on these assumptions, an average UC center would be expected to be revenue positive from the addition of tympanometry within the first month of implementation (29.4 days) and generate $4,862 in gross revenue monthly in perpetuity exclusively from the additional CPT billing related to tympanometry.
Discussion
The results of this retrospective UC cohort study suggest that a regression model trained on a large data set of de-identified UC encounters can predict cases where tympanometry would have clinical utility with high accuracy. The combination of the model’s high accuracy and the level of agreement between expert labelers suggests that this approach could have clinical utility in guiding staff on the appropriate application of tympanometry. Therefore, such a prediction tool could be valuable in UC, ED, and primary care settings, where staff are unlikely to have familiarity with the indications for tympanometry.
The predicted utilization rate of tympanometry was 18% based on the model’s application to a large sample of real-world UC cases. The model predicted tympanometry may provide clinically valuable data in nearly one-fifth of encounters. Given the poor test characteristics of standard otoscopy, rule-based application of tympanometry has the potential to standardize care and improve antibiotic stewardship.6 Additionally, visually subtle cases of OME may be identified and otolaryngology referrals placed more appropriately and expeditiously. Given the frequency with which ear and hearing complaints were seen among this real-world UC encounter set, it appears that tympanometry has the potential to meaningfully affect patient safety and resource utilization.
Additionally, the financial modeling estimate suggests that tympanometry could support revenue to reach the “break-even” point within 1 month when applied in an average hypothetical UC setting. Finally, to our knowledge, this is the first study to date describing the frequency of common chief complaints and diagnoses in a general UC population.
Limitations
This study has several limitations worth noting. First, the retrospective design and use of de-identified encounters prevented correlation with actual otoscopic findings, which limits the ability to verify predicted tympanometry indications by otoscopy exam results. Second, the model’s performance was validated using expert review rather than patient outcomes due to the study design; this could somewhat overestimate real-world utility. Third, financial model predictions were based on assumptions from published reimbursement data, fee-for-service billing, and current device pricing rather than prospective implementation. It is possible that individual organizations may realize different levels of reimbursement based on their specific payer mix and contracts. Finally, while the model we developed identified cases likely to have a justifiable indication for tympanometry, it is possible that it overestimates real-world use as clinician discretion and/or patient preference to forgo tympanometry may occur for myriad reasons. These limitations could be addressed in future studies designed to prospectively validate the model and assess operational feasibility testing in a diverse range of UC environments.
Conclusion
Tympanometry is a simple, yet underutilized tool in UC despite strong evidence and guidelines supporting its diagnostic value for common UC complaints. This retrospective modeling analysis suggests that an ML algorithm could operate in lieu of specialty expertise in guiding the appropriate application of tympanometry in UC. The financial analysis indicates that, if applied in an average UC center, the addition of tympanometry could transition to revenue positive within 30 days. Future work should prospectively validate this model to evaluate effects on patient-oriented outcomes and rates of inappropriate otolaryngology referral and antibiotic use.
Manuscript submitted November 11, 2025; accepted April 8, 2026.
References
- [1]. Feldman AS. Tympanometry: application and interpretation. Ann Otol Rhinol Laryngol. 1976;85(2 Suppl 25 Pt 2):202-208. doi:10.1177/00034894760850S238
- [2]. Onusko E. Tympanometry. Am Fam Physician. 2004 Nov 1;70(9):1713-20
- [3]. Alencar AP, Iório MC, Morales DS. Equivalent volume: study in subjects with chronic otitis media. Braz J Otorhinolaryngol. 2005 Sep;71(5):644-8.
- [4]. Rosenfeld RM, Shin JJ, Schwartz SR, et al. Clinical Practice Guideline: Otitis Media with Effusion (Update). Otolaryngol Head Neck Surg. 2016;154(1 Suppl):S1-S41. doi:10.1177/0194599815623467
- [5]. Erkkola-Anttinen N, Tähtinen PA, Laine MK, Ruohola A. Parental role in the diagnostics of otitis media: can parents be taught to use tympanometry reliably? Int J Pediatr Otorhinolaryngol. 2014 Jul;78(7):1036-9.
- [6]. Abbott P, Rosenkranz S, Hu W, Gunasekera H, Reath J. The effect and acceptability of tympanometry and pneumatic otoscopy in general practitioner diagnosis and management of childhood ear disease. BMC Fam Pract. 2014 Dec 12;15:181
- [7]. American Association of Medical Assistants. State scope of practice laws. State Scope of Practice Laws. Accessed October, 12, 2025. https://www.aama-ntl.org/publications/state-scope-of-practice-laws
- [8]. Yaffe NM, Quereshy HA, Quinton BA, Otteson TD, Shah JR. Reimbursement Trends in Pediatric Otolaryngology From 2000 to 2020: A CMS Physician Fee Schedule Analysis. Otolaryngol Head Neck Surg. 2023;168(1):59-64. doi:10.1177/01945998221091697
- [9]. Burvenich R, Dillen H, Trinh NTH, et al. Antibiotic use in ambulatory care for acutely ill children in high-income countries: a systematic review and meta-analysis. Arch Dis Child. 2022;107(12):1088-1094. doi:10.1136/archdischild-2022-324227
- [10]. McWilliams DB, Jacobson RM, Van Houten HK, Naessens JM, Ytterberg KL. A Program of Anticipatory Guidance for the Prevention of Emergency Department Visits for Ear Pain. Arch Pediatr Adolesc Med. 2008;162(2):151–156
- [11]. Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013;131(3):e964-e999.
- [12]. Jones WS, Kaleida PH. How helpful is pneumatic otoscopy in improving diagnostic accuracy? Pediatrics. 2003 Sep;112(3 Pt 1):510-3.
- [13]. Brinker DL Jr, MacGeorge EL, Hackman N. Diagnostic Accuracy, Prescription Behavior, and Watchful Waiting Efficacy for Pediatric Acute Otitis Media. Clin Pediatr (Phila). 2019 Jan;58(1):60-65. doi: 10.1177/0009922818806312. Epub 2018 Oct 12. Erratum in: Clin Pediatr (Phila). 2019 Apr;58(4):491
- [14]. Gerber JS, Prasad PA, Russell Localio A, Fiks AG, Grundmeier RW, Bell LM, Wasserman RC, Keren R, Zaoutis TE. Variation in Antibiotic Prescribing Across a Pediatric Primary Care Network. J Pediatric Infect Dis Soc. 2015 Dec;4(4):297-304
- [15]. Rosenfeld RM, Tunkel DE, Schwartz SR, et al. Clinical Practice Guideline: Tympanostomy Tubes in Children (Update). Otolaryngol Head Neck Surg. 2022;166(1_suppl):S1-S55. doi:10.1177/01945998211065662
- [16]. Paradise JL, Rockette HE, Colborn DK, Bernard BS, Smith CG, Kurs-Lasky M, Janosky JE. Otitis media in 2253 Pittsburgh-area infants: prevalence and risk factors during the first two years of life. Pediatrics. 1997 Mar;99(3):318-33
- [17]. Ramgopal S, Aronson PL, Marin JR. United States’ Emergency Department Visits for Fever by Young Children 2007-2017. West J Emerg Med. 2020;21(6):146-151. Published 2020 Oct 27. doi:10.5811/westjem.2020.8.47455
- [18]. Taziki MH, Behnampour N. A study of the etiology of referred otalgia. Iran J Otorhinolaryngol. 2012;24(69):171-176.
- [19]. Cox KW. Temporomandibular disorder and new aural symptoms. Arch Otolaryngol Head Neck Surg. 2008 Apr;134(4):389-93. doi: 10.1001/archotol.134.4.389. PMID: 18427004.
- [20]. Keersmaekers K, De Boever JA, Van Den Berghe L. Otalgia in patients with temporomandibular joint disorders. J Prosthet Dent. 1996 Jan;75(1):72-6.
- [21]. Lai D, Li W, Xian J, Liu S. Multifrequency tympanometry in adults with otitis media with effusion. Eur Arch Otorhinolaryngol. 2008;265(9):1021-1025. doi:10.1007/s00405-008-0705-x
- [22]. Chandrasekhar SS, Tsai Do BS, Schwartz SR, et al. Clinical Practice Guideline: Sudden Hearing Loss (Update). Otolaryngol Head Neck Surg. 2019;161(1_suppl):S1-S45. doi:10.1177/0194599819859885
- [23]. Klein L, Handzel O, Shilo S, Oron Y, Abu Eta R, Muhanna N, Ungar OJ. Is Sudden Sensorineural Hearing Loss an Otologic Emergency? Evidence-Based Cutoff for Optimal Treatment Initiation for Sudden Unilateral Sensorineural Hearing Loss: A Case Series and Meta-Analyses. Otol Neurotol. 2023 Mar 1;44(3):216-222
- [24]. Nelson L, et al. The Impact of Intratympanic Steroid Dosage on Hearing Recovery in Sudden Sensorineural Hearing Loss. Ann Otol Rhinol Laryngol. 2023 Aug;132(8):879-887
- [25]. Osafo NK, Friedland DR, Harris MS, Adams J, Davis C, Osinski K, Tong L, Luo J. Standardization of Outcome Measures for Intratympanic Steroid Treatment for Idiopathic Sudden Sensorineural Hearing Loss. Otol Neurotol. 2022 Dec 1;43(10):1137-1143.
- [26]. Sahni NR, Carrus B. Artificial intelligence in U.S. health care delivery. N Engl J Med. 2023;389(4):348-358. doi:10.1056/NEJMra2204673
- [27]. R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2023. Accessed April 21, 2026. https://www.R-project.org/
- [28]. MAICO Diagnostics. easyTymp Handheld Screening Tympanometer. MAICO Diagnostics. Accessed February 22, 2026. https://maico-diagnostics.com/products/easytymp
- [29]. Urgent Care Association. 2021 Benchmarking Report: Summer 2021. Published 2021. Accessed April 21, 2026. https://urgentcareassociation.org/wp-content/uploads/2023/04/UCA-Benchmarking-Report-Summer-2021.pdf
Author Affiliations: Jeff Lacour, MD, North Oaks ENT and Allergy, Hammond, Louisiana; Compassio Medical Education, Covington, Louisiana; MAICO Diagnostics, Minneapolis, Minnesota. John Weissert, Intellivisit, UCP-Merchant Medicine, Minneapolis, Minnesota. Dan Frankowski, Boxydog, Minneapolis, Minnesota. Demetrio Aguila III, MD, Total Pain Solutions, Atkinson, Nebraska. Joshua Russell, MD, Intellivisit, UCP-Merchant Medicine, Minneapolis, Minnesota. Disclosures: Dr. Lacour reports serving as an educator for MAICO Diagnostics. Mr. Weissert reports relationships with Intellivisit and UCP-Merchant Medicine. Mr. Frankowski reports a relationship with Boxydog. Dr. Aguila reports a relationship with Total Pain Solutions. Dr. Russell reports relationships with Intellivisit and UCP-Merchant Medicine. All relevant financial relationships have been reviewed and mitigated to ensure balance and absence of commercial bias.
