Published on
Differential Diagnosis
- Sinus tachycardia
- Supraventricular tachycardia
- Ventricular tachycardia
- Inferior STEMI
- Atrial fibrillation with rapid ventricular response (RVR)
Diagnosis
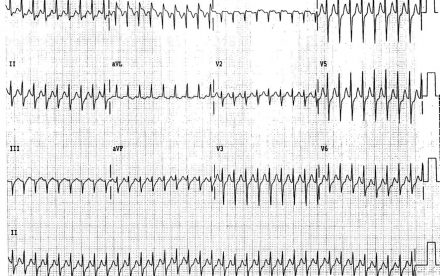
The ECG reveals a narrow complex rhythm, so this is not ventricular tachycardia (which would be wide complex). The rhythm is regular, excluding the diagnosis of atrial fibrillation. There are no p waves, so sinus tachycardia is very unlikely. Inferior STEMI is not present, as there are no ST elevations in the inferior leads of II, III, aVF. This ECG shows supraventricular tachycardia.
Learnings
- Supraventricular tachycardia usually occurs from AV node reentry
- The ECG will show a narrow-complex tachycardia
- It is most often seen in women, usually in young adults
- It is unusual to have concomitant cardiovascular disease
- Symptoms may include palpitations, lightheadedness, shortness of breath, or chest discomfort
Pearls for Initial Management and Considerations for Transfer
- Vagal maneuvers may be effective
- A new technique called “postural modification” has recently been described,where the patient lays supine while a vagal maneuver is being performed (such as holding the breath and bearing down) as the extended legs are raised quickly to
- 45 degrees by the provider
- If available, adenosine 6 mg IV over 1-3 seconds followed by 20 mL NS bolus can be used when vagal maneuvers fail. Monitoring capability, ACLS preparedness and physician supervision is necessary
- Transfer should be initiated with hypotension, confusion, inability to terminate the rhythm, or diagnostic uncertainty
A 62-Year-Old Woman with Dizziness and Palpitations
1 2