Published on
Download the article PDF: Clinical Image Challenges January 2026
Differential Diagnosis
- Anterior ST-elevation myocardial infarction (STEMI)
- Left ventricular aneurysm
- Pericarditis
- Myocarditis
- Brugada syndrome
Diagnosis
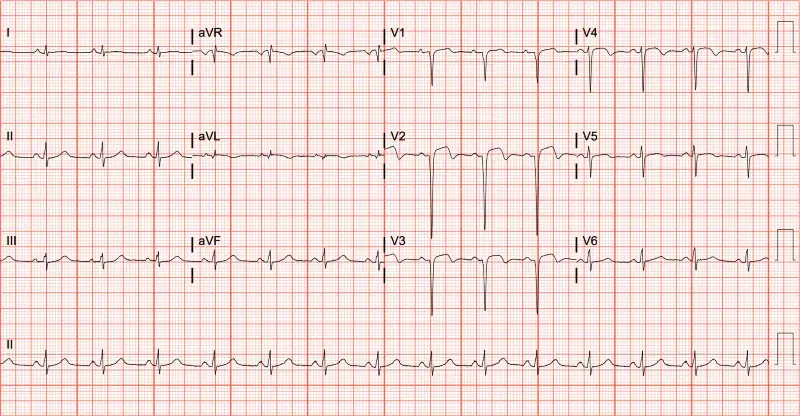
The diagnosis in this case is left ventricular aneurysm. The ECG shows ST elevation in V1-4, deep Q-waves and an absence of reciprocal ST-depressions—taken together, these findings are consistent with left ventricular (LV) aneurysm.1 First described angiographically in 1951, LV aneurysm is an outpouching or weakening of the apical ventricular wall frequently seen more than two weeks after an acute MI, with prevalence as high as 35-64% in the absence of reperfusion therapy.2-3
Electrocardiographically, the ST-elevation morphology seen in the precordial leads persists more than 2 weeks after an MI, rather than being dynamic as in anterior STEMI. The ECG may show either concave or convex morphology of the ST elevation and deep Q waves (Figure 2). LV aneurysm is commonly misinterpreted as acute MI; therefore, it is imperative that clinicians familiarize themselves with the key features.4

One method of distinguishing LV aneurysm from anterior STEMI involves analysis of the T/QRS ratio.5 LV aneurysms exhibit T-waves with smaller amplitudes relative to the QRS complexes than STEMIs. A T/QRS ratio greater than 0.36 (T wave amplitude compared with QRS amplitude) in any single precordial lead favors anterior STEMI while T/QRS ratio less than 0.36 in all precordial leads favors the diagnosis of LV aneurysm (Figure 3). STEMI is more likely if there are dynamic ECG changes or new ST changes when compared with prior ECGs.6 It is important to keep the clinical context in mind, as high clinical concern (eg, crushing chest pain, diaphoretic, ill-appearing) favors STEMI.

In pericarditis, diffuse ST elevation is often seen along with PR depressions. There may also be PR elevation in aVR and sometimes V1. In the example provided, the ST-elevations are focal to the anterior leads, making pericarditis unlikely.
Myocarditis can cause ST elevation but is typically non-specific. Sinus tachycardia is the most common ECG finding in myocarditis. Myocarditis is often seen after a recent viral illness, autoimmune conditions (eg, systemic lupus erythematous), or after certain medication administration (eg, anti-monoclonal antibodies), so clinical correlation is important.
Brugada syndrome involves ST-elevation in V1-V3, with subsequent negative T-wave in association with ventricular dysrhythmia (or a clinical context suggestive of, eg, syncope or sudden cardiac death).
What To Look For
- Look for ST elevations in the precordial leads (V1-V4) with deep Q-waves, and without reciprocal ST depressions.
- The ST segments (with LV aneurysm) are not dynamic and are similar to prior ECGs.
- A high T/QRS ratio >0.36 in any single precordial lead favors acute MI over LV aneurysm, while T/QRS ratio less than 0.36 in all precordial leads favors LV aneurysm.
Pearls For Initial Management, Considerations For Transfer
- The presence of electrocardiographic findings of LV aneurysm suggests a prior MI, and these are high-risk patients; therefore, the urgent care physician should have a low threshold for emergency department referral even if the electrocardiographic findings are unchanged.
- Serial ECGs to assess for dynamic changes can be helpful to determine the urgency of emergency department referral.
References
- ECG Stampede. Left ventricular aneurysm. https://www.ecgstampede.com/glossary/left-ventricular-aneurysm/#:~:text=Left%20ventricular%20aneurysm%20is%20characterized,absence%20of%20reciprocal%20ST%20depressions. Accessed August 1, 2025.
- Mills RM, Young E, Gorlin R, et al. Natural history of S-T segment elevation after acute myocardial infarction. Am J Cardiol. 1975;35:609-614.
- Meizlish JL, Berger HJ, Plankey M, et al. Functional left ventricular aneurysm formation after acute anterior transmural myocardial infarction. Incidence, natural history, and prognostic implications. N Engl J Med. 1984;311:1001-1006.
- Brady WJ, Perron AD, Ullman EA, et al. Electrocardiographic ST-segment elevation: correct identification of acute myocardial infarction (AMI) and non-AMI syndromes by emergency physicians. Am J Emerg Med. 2001;19(1):79-80.
- Smith SW. T/QRS ratio best distinguishes ventricular aneurysm from anterior myocardial infarction. Am J Emerg Med. 2005;23(3):279-287. doi:10.1016/j.ajem.2005.01.003.
- Klein LR, Shroff GR, Beeman W, Smith SW. Electrocardiographic criteria to differentiate acute anterior ST-elevation myocardial infarction from left ventricular aneurysm. Am J of Emer Med. 2015;33(6):786-790. Doi:10.1016/j.ajem.2015.03.044.