Published on
Differential Diagnosis
- Benign early repolarization
- Hyperkalemia
- de Winter T waves
- ST-elevation Myocardial Infarction (STEMI)
- Brugada syndrome
Diagnosis
The patient was diagnosed with de Winter T waves. The ECG reveals a normal sinus rhythm with a rate of 72 beats per minute. There are tall, symmetrical T waves with upsloping ST depressions in the precordial leads, as well as ST segment elevation in aVR. When compared to the amplitude of the QRS complex, the precordial T waves are large, particularly in leads V4 and V5.
The pattern seen here is called de Winter T waves or de Winter syndrome. Described in 2008 by de Winter, this pattern of upsloping ST depressions and hyperacute T waves in the precordial leads suggests proximal left anterior descending (LAD) occlusion.1 While this pattern does not meet classic STEMI criteria, it does suggest the presence of an occlusion myocardial infarction (OMI) that warrants emergent reperfusion. This pattern is seen in just 2% of acute LAD occlusions and is often misdiagnosed.2 Widely considered an anterior STEMI equivalent, cath lab activation for the de Winter pattern is recommended just as with a classic STEMI pattern.3
The full characterization of the typical de Winter pattern is as follows:
- 1 to 3 mm upsloping ST depression at the J point in precordial leads
- Large symmetrical T waves in precordial leads
- Narrow or slightly widened QRS complex
- 1 to 2 mm ST-segment elevation in aVR
- Loss of precordial R wave progression in some patients1
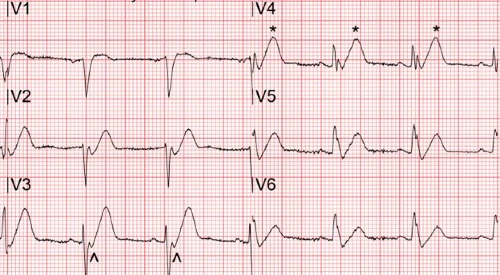
Large T waves occur in many conditions including hyperkalemia, benign early repolarization, and ischemia. Large T waves found in patients with ischemia, called hyperacute T waves, are symmetric and broad based, with an amplitude that is relatively large compared to the size of the QRS complex. Conversely, hyperkalemia causes peaked T waves with a narrow base and a pointed peak. Benign early repolarization is diagnosed with diffuse, concave up ST segment elevation, as opposed to the ST segment depression seen here.
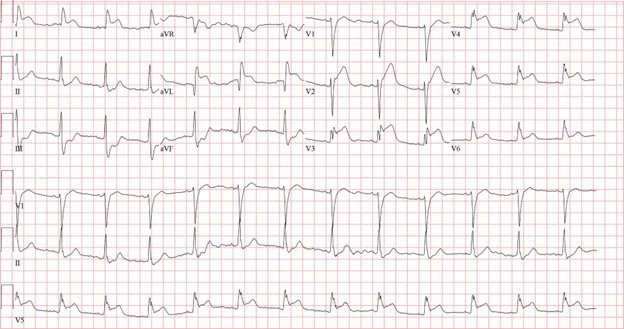
Hyperacute T waves are found in early ischemia, and often precede ST segment elevation. De Winter T waves share many similarities with hyperacute T waves, but the de Winter pattern was originally described as static, persisting until reperfusion. The broad, symmetric T waves of the de Winter pattern may persist for hours or days without evolving into an overt STEMI, which adds to the complexity of making this diagnosis. In the case of this patient, repeat ECG after EMS arrival revealed ST elevation consistent with STEMI (Figure 3).
Learnings/what to look for:
- Tall, prominent, symmetrical T waves with upsloping ST depression in the precordial leads should prompt consideration of de Winter T waves.
- Repeat ECGs in patients with this pattern may remain static or progress to STEMI.
Pearls for initial management and considerations for transfer:
- The de Winter pattern is seen in just 2% of acute LAD occlusions and is often under-recognized. While this pattern does not fit classical STEMI criteria, these patients need emergent reperfusion and should be transferred immediately for cath lab activation.
- Recognizing this pattern and expediting transfer will save the life of your patient.
References
- de Winter RJ, Verouden NJ, Wellens HJ, Wilde AA. A new ECG sign of proximal LAD occlusion. N Engl J Med. 2008 Nov 6;359(19):2071-3
- Verouden NJ, Koch K T, Peters R J, et al. Persistent precordial “hyperacute” T-waves signify proximal left anterior descending artery occlusion. Heart. 2009;95(20):1701–6. doi: 10.1136/hrt.2009.174557.
- Rokos IC, French WJ, Mattu A, Nichol G, Farkouh ME, Reiffel J, et al. Appropriate cardiac cath lab activation: optimizing electrocardiogram interpretation and clinical decision-making for acute ST-elevation myocardial infarction. Am Heart J. 2010;160(6):995–1003.