Published on
Download the article PDF: Clinical Image Challenges October 2025
Differential Diagnosis
- Normal early intrauterine pregnancy
- Ectopic pregnancy
- Heterotopic pregnancy
- Gastrointestinal causes (eg, constipation, diverticulitis)
- Urinary tract infection
- Ureterolithiasis
- Ovarian cyst or mass
Diagnosis
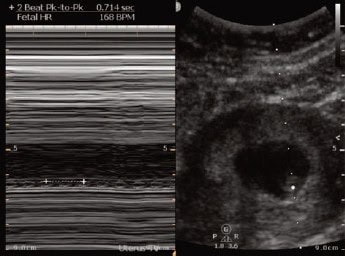
Transabdominal POCUS revealed an intrauterine gestational sac containing a fetal pole with a crown-rump length (CRL) measurement of 1.61 cm, consistent with an 8 week and 0 day gestation. M-mode (motion mode) imaging confirmed fetal cardiac activity with a fetal heart rate (FHR) of 168 beats per minute (bpm). No adnexal masses or free fluid were seen. The POCUS findings confirmed a live intrauterine pregnancy. Based on this, the provider was able to safely exclude ectopic pregnancy, avoiding an emergency department (ED) referral, and instead provided outpatient obstetrics-and- gynecology follow-up.

Discussion
Abdominal pain in early pregnancy, even if mild and without bleeding, warrants evaluation for ectopic pregnancy. Visualization of an intrauterine pregnancy (IUP) essentially excludes ectopic pregnancy in patients without risk factors for heterotopic pregnancy, which is the simultaneous occurrence of an intrauterine and an ectopic pregnancy.1,2 IUP is confirmed when the intrauterine gestation sac contains either a yolk sac or a fetal pole.3 Heterotopic pregnancy, while rare (incidence of 1 in 30,000 spontaneous pregnancies), must be considered in patients with the following characteristics:
- Actively receiving assisted reproductive technologies (ART)
- Prior ectopic pregnancy
- Pelvic inflammatory disease
- Tubal surgery or pathology
- Endometriosis
The incidence increases to 0.9 to 1% in patients undergoing ART.4 POCUS was critical in confirming an IUP and thus excluding ectopic pregnancy in our patient without any heterotopic pregnancy risk factors.
On transabdominal ultrasound, a yolk sac, the earliest definitive sign of an IUP, is typically visible around 6.5-7 weeks of gestation when the mean gestational sac diameter is at least 20 mm. A fetal pole and cardiac activity usually become visible after 7 weeks on transabdominal ultrasound, and at 6 weeks on transvaginal ultrasound.4
In our patient, fetal pole and cardiac activity were both seen, placing the pregnancy at a minimum of 7 weeks of gestation. CRL measurement dated the pregnancy to approximately 8 weeks and 0 days of gestation. FHR of 168 bpm was measured using M-Mode and fell within the normal range for an 8-week gestation.5 The normal range of fetal heart rate during the first trimester is approximately 110–180 bpm, with the lower end seen at the earliest detection and the upper end peaking around 8–9 weeks of gestation.5,6 In this case, POCUS was used to confirm an IUP, thus essentially ruling out an ectopic pregnancy and avoiding ED referral.
What to Look For
- Intrauterine gestational sac containing a yolk sac or a fetal pole confirms an IUP.
- Measurement of CRL estimates the gestation age.
- The presence of free fluid in the pelvis or an adnexal mass should raise suspicion for ectopic pregnancy.
Pearls for Urgent Care Management
- Evaluate all reproductive-age women with abdominal pain for pregnancy.
- Patients undergoing fertility treatment are at increased risk for heterotopic pregnancy and should be evaluated with same-day transvaginal ultrasound and referred for gynecologic follow-up if they present with abdominal pain, even when an IUP is identified.
- In well-appearing patients with a confirmed IUP on transabdominal POCUS and no risk factors for heterotopic pregnancy, ED transfer is often unnecessary.
References
- American College of Emergency Physicians. Emergency ultrasound guidelines. Ann Emerg Med. 2009;53(4):550-570. doi:10.1016/j.annemergmed.2008.12.013
- American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Early Pregnancy:, Hahn SA, Promes SB, Brown MD. Clinical Policy: Critical Issues in the Initial Evaluation and Management of Patients Presenting to the Emergency Department in Early Pregnancy [published correction appears in Ann Emerg Med. 2017 Nov;70(5):758. doi: 10.1016/j.annemergmed.2017.03.035.]. Ann Emerg Med. 2017;69(2):241-250.e20. doi:10.1016/j.annemergmed.2016.11.002
- Doubilet PM, Benson CB, Bourne T, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369(15):1443–1451. doi:10.1056/NEJMra1302417
- Rowling SE, Langer JE, Coleman BG, Nisenbaum HL, Horii SC, Arger PH. Sonography during early pregnancy: dependence of threshold and discriminatory values on transvaginal transducer frequency. AJR Am J Roentgenol. 1999;172(4):983-988. doi:10.2214/ajr.172.4.10587132
- Ouyang Y, Qin J, Lin G, Xiang S, Li X. Reference intervals of gestational sac, yolk sac, embryonic length, embryonic heart rate at 6-10 weeks after in vitro fertilization-embryo transfer. BMC Pregnancy Childbirth. 2020;20(1):533. Published 2020 Sep 14. doi:10.1186/s12884-020-03186-2
- Araujo Júnior E, Costa RS, Fonseca BC, Martins WP, Pires CR, Zanforlin Filho SM. Reference intervals of embryos/fetuses heart rate between 6 and 14 weeks of pregnancy. J Matern Fetal Neonatal Med. 2014;27(13):1385-1388. doi:10.3109/14767058.2013.856416
Case provided by Tatiana Havryliuk, MD, emergency physician in New York, New York, and founder of Hello Sono.