Published on
Urgent message: Mechanism of injury – in case being thrown from a slow-moving vehicle – provides essential clues to the extent of injuries, even if the patient initially thought them to be relatively minor. Proper evaluation requires a thorough history.
Shannon Dowler, MD
The Case
The patient is a 23-year-old female who presented to urgent care with an approximately 36-hour history of “shoulder pain.” She is otherwise well-appearing.
Discussion with the patient reveals that she was riding as a passenger in a Jeep with the doors off when she took her seatbelt off as they rounded the final curve to her garage. She fell out of the Jeep onto the ground while the car was still moving, reportedly at approximately 10 miles per hour.
The patient reports that she fell onto her left side and that her only injuries – or so she thought at the time – was some “road burn” along her left arm and shoulder.
She did not seek medical attention at the time.
The patient went to bed that night and woke up “sore” the next day. Her pain persisted throughout the day, through the time she was encountered in the exam room, 36 hours after being thrown from the vehicle.
Observations and Findings
Evaluation of the patient revealed the following:
PMH: No chronic illnesses and no history of fractures
Meds: Oral contraceptives
Allergies: None
FH: Noncontributory
SH: Alcohol was involved in the accident, but the patient was not driving.
- Nonsmoker
- Student
- No recreational drugs
ROS: Complaining of pain with lifting her left shoulder “in front” and “on the side.” Denies any head trauma. Denies any chance of pregnancy. No cough, chest pain, or shortness of breath. Essentially negative ROS except for upper extremity pain.
PE: T: 98.7; BP: 126/80; HR: 79; RR: 16
Gen: Pleasant, well-appearing young female in no acute distress; alert and oriented x3.
Ext: Superficial abrasions noted on forearm and over deltoid area without signs of infection; exam of shoulder reveals no bony deformity and no focal bony tenderness to palpation though discomfort over AC joint and lateral deltoid; no neurologic or vascular deficits; active ROM markedly diminished but passive ROM reveals 50% extension and abduction limited due to pain.
CV: NSR without m/r/g
Pulm: CTAB without w/r/r
X-rays: See figures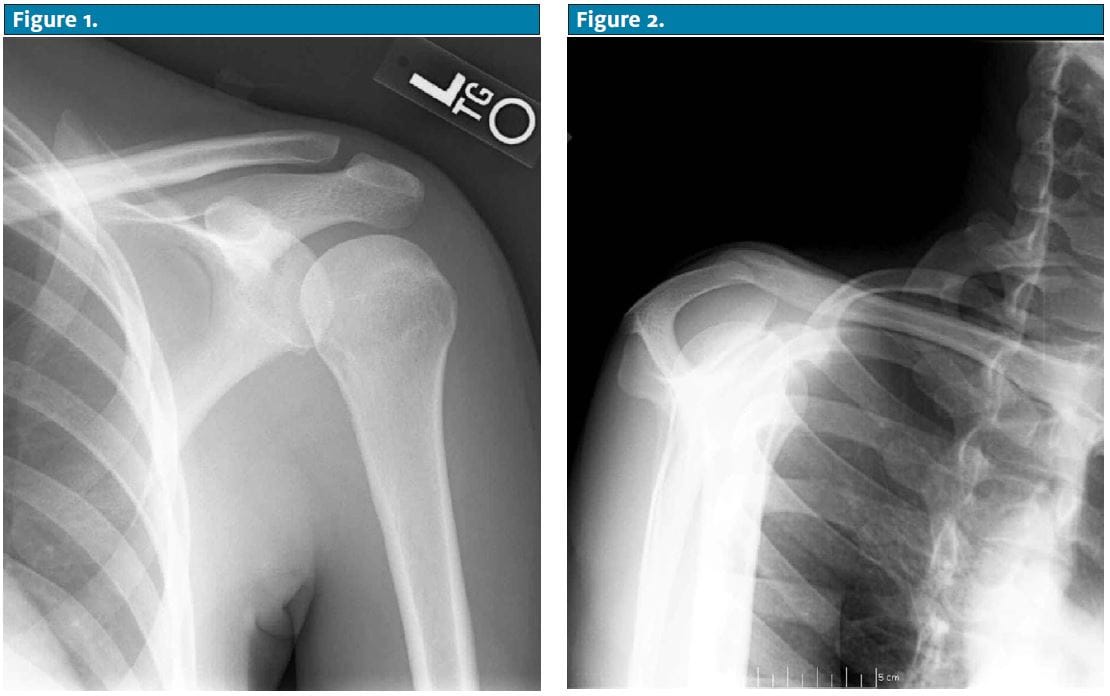
Diagnosis
The patient has a non-displaced fracture through the body of the scapula. Confirmation with CT revealed “non-displaced vertically oriented fracture of the scapula involving the body of the scapula, scapular spine and supraspinatus portion of the scapula.”
There was no evidence of glenoid fossa, acromion, or coracoid process involvement; the AC joint was intact.
No visualized associated humerus or rib fractures seen.
Discussion
Scapular fractures are usually associated with significant traumas, most typically resulting from motor vehicle injuries and pedestrian-MV injuries. The clinician should be alert to other associated injuries (e.g., clavicle, rib, spine, pulmonary, abdominal injuries).
If the patient is stable and has no other associated injuries and pain can be controlled on an outpatient basis, shoulder immobilization and narcotic analgesia with referral to orthopedics on an outpatient basis is a reasonable approach to management.
CT scan is generally recommended to assess for degree of displacement because surgical fixation is indicated with > 1 cm medical displacement or > 40° angulation.
