Published on
Urgent message: Urgent care is well established as an appropriate destination for many patients whose symptoms are not being limb- or life-threatening. When a truly emergent case presents, however, we need to provide immediate care and assess whether the patient can receive optimal care on site or needs transfer to higher-acuity setting.
Deb Rogers, DO and Douglas A. Rund, MD, FACEP, FAEMS
Cowboys of medicine? We are able to diagnose and manage almost all complaints at the bedside with our history and exam, but what happens when the emergency presents? We all know that patient—a well-intentioned soul who has been putting their symptoms on the back burner and is now fighting off the sickle with all of their might.
Why didn’t they just go straight to the ED?
While we can provide care for varied symptoms, we do have certain limitations; room 3 is not an interventional cardiology suite, and it is probably best to use that BIC pen to sign prescriptions instead of performing an emergent tracheostomy!
When the emergency presents, the patient will need rapid assessment, stabilization, and preparation for transfer to the best available facility. We need to rapidly recognize the acuity, and quickly make a decision: Can the patient be transported by private car, private ambulance, or advanced life support (ALS)-capable emergency medical services (EMS)? And do we recommend emergency transport with “lights and sirens”? Appropriate decisions on mode and speed of transfer can have profound implications on outcomes.
Common Presentations/Indications Requiring Transfer
So, which patients with which conditions do we transport? The short answer is, anyone with a condition that we cannot handle at the facility or anyone who needs hospital admission. However, transport can have many different meanings. For example, the man with nonemergent epistaxis may be able to travel by private car to the ENT office for follow-up, while the woman with STEMI will need to go straight to an interventional cardiology suite. In general, our disposition decisions could include the following:
- Early follow-up with the patient’s primary care physician
- Early follow-up with a specialist
- Urgent care-ordered lab or radiologic testing with urgent care follow-up for test results
- Admission to a specialized facility
- Urgent transfer to an emergency department
- Emergent transfer to an emergency department
It’s all easier said than done. For example, what seems like a simple muscular strain could actually be a deep vein thrombosis (DVT). A seemingly obvious diagnosis of chest wall strain could actually be a thoracic aortic dissection. The balance of over-transferring vs sending a patient home for outpatient follow-up can sometimes be difficult and represent a fine line. Here, we explore conditions with possible diagnoses ranging from benign to life-threatening, with focus on chest pain, stroke, sepsis, shortness of breath, extremity pain, trauma, abdominal pain, and acute change in mental status.1
Time-Sensitive Conditions
Emergency medical technicians (EMTs) and paramedics are taught that the truly emergent conditions are myocardial infarction, stroke, sepsis, and major trauma. Because earliest possible definitive treatment is lifesaving, immediate, emergent transport to the most appropriate facility is outlined in most EMS protocols.
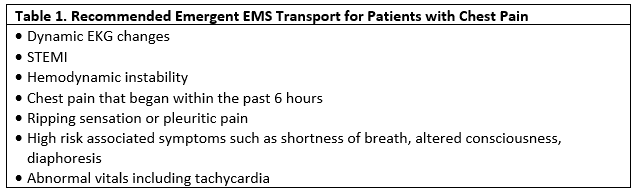
Chest Pain
Let’s start with chest pain. The life-threatening conditions are myocardial infarction, thoracic aortic dissection pulmonary embolism, and tension pneumothorax. In some respects, the STEMI is our easiest case; the patient has classic chest tightness radiating to the jaw or arms and the ECG shows ST-segment elevation. Emergent transfer directly to the catheterization suite to open the arterial blockage is the clear choice. But what about atypical symptoms? Diabetic patients may have diminished pain sensitivity. Women may present with atypical symptoms such as shortness of breath, fatigue, epigastric pain, nausea, or sleep disturbances, or pain in the right shoulder.
A good argument can be made that virtually all adult patients with chest pain deserve an evaluation with a 12-lead ECG. But what about the patient with those vague chest pains and a normal or nonspecific 12-lead ECG? A non-STEMI may well be lethal but could be overlooked if the ECG alone is considered. Calculation of a risk score for acute coronary syndrome is the best option in such cases. High-yield risk scores include age, sex, cardiovascular risk factors, and chest pain characteristics.2,3
Of course, patients often have more benign causes of chest pain, such as chest wall strain from coughing, esophageal reflux, or conditions such as herpes zoster, where the pain may precede the development of rash. Pain that tends to suggest a more benign cause can be pleuritic, sharp, related to cough, localized with one finger, reproduced by palpation, fleeting pain lasting a few seconds or less, or pain radiating into the lower extremities. As with all potentially worrisome symptoms, the most helpful question is, “Why did you seek treatment now? What changed?” Adults with new-onset or markedly worsened chest pain deserve an appropriate evaluation, including an assessment of risk factors for myocardial infarction.
Physical assessment usually begins with the physician taking a quick look at the patient’s general appearance and determination if the patient looks “sick” or “not sick.” Experienced clinicians can usually make this determination quickly. Is the patient pale, ashen, gasping for breath, or in excruciating pain? Review of the vital signs is next, and any abnormal vital sign must be explained. In cases of chest pain, tachycardia is a hallmark of pulmonary embolism but may be associated with myocarditis or tachyarrhythmia. Paramedics will measure pulse oximetry in patients with chest pain. Low PO2 can be associated with pulmonary embolism, pneumonia, bronchoconstriction, or congestive heart failure.
Stroke
The treatment of thrombotic stroke has evolved so rapidly in recent years that earliest possible CT scan and transfer to the endovascular suite in a comprehensive stroke center gives the patient a chance for full recovery. Most EMS providers evaluate patients with suspected stroke with one of the following scales:
- Cincinnati Pre-hospital Stroke Scale (speech, facial droop and arm drift)
- Los Angeles Motor Scale (LAMS)
- Miami Emergency Neurologic Deficit (MEND)
The LAMS scale evaluates facial droop, arm drift, and grip strength. The Cincinnati scale and LAMS look for evidence of large cerebral vessel occlusion; thus, the need for earliest possible endovascular intervention if such is available in a reasonable time frame. The MEND exam is a miniaturized version of the NIH stroke scale and is available in an iPhone app that allows the provider to calculate the score and get a final written summary immediately.
Stroke mimics can be caused by hypoglycemia, Bell’s palsy, or a Todd’s paralysis following a seizure. Paramedics are expected to obtain a blood glucose in every patient with suspected stroke. For thrombotic stroke. current guidelines suggest that TPA be given within 4.5 hours of stroke symptom onset.4 A patient with symptoms suggesting a stroke and within the TPA window should be transported by EMS emergency traffic to a stroke center. Interventional therapy can lengthen this time frame up to 6-12 hours.5
Sepsis
The third time-critical illness in EMS is sepsis, a life-threatening condition. Suspicion of sepsis is a first step in its recognition. Does the patient have fever, tachycardia, and elevated respiratory rate? Is there a suspected source of infection (urinary tract infection, pneumonia, or decubiti)? Is the patient immunocompromised and/r elderly? EMS personnel are trained to have a low threshold for suspecting sepsis, to treat with large volumes of intravenous fluids, and call a “sepsis alert” to the receiving facility.
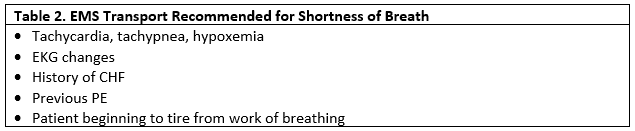
Shortness of Breath
Shortness of breath also has a wide range of presentations and complications. A 10-year-old with asthma on exertion that ran out of their inhaler a week ago and who is in minimal distress can likely be treated and sent home after symptom resolution. However, that same child in moderate distress with no resolution after ipratropium bromide (Atrovent)/albuterol aerosol will, in all likelihood, need EMS transport to a facility that handles pediatric patients. If the patient can be stabilized and will likely need admission, it is important to ensure the receiving facility admits pediatric patients. However, if stabilization isn’t achieved at the urgent care center, then transfer to the closest emergency department is the best option.
Extremity Pain
Whether traumatic or infectious, extremity pain is a common complaint that can quickly become complicated. Mild cellulitis in an otherwise healthy patient could be treated with a quick antibiotic prescription and follow-up with a primary care physician. However, the same patient with crepitus suggesting a necrotizing soft tissue infection (NSTI) needs to be transported by EMS for surgical debridement. Some conditions that will also require EMS transport include extremity symptoms of intractable pain, open fracture, compartment syndrome, or consideration of NSTI.
Minor Trauma
We are capable of managing most minor traumas on site, followed by referral (“treat and street”). Fortunately, new guidelines help in the evaluation of extremity injury. These include the Ottawa foot and ankle rules, which decrease imaging in ankle injuries and show a “decrease in ankle radiography, waiting times, and costs without an increased rate of missed fractures.”6 The Canadian C-Spine rules or NEXUS criteria help decrease imaging of the C-spine.7,8
Sometimes patient circumstances determine the urgency and need for transport. For example, an elderly patient who is taking an anticoagulant who falls and sustains a head injury (even seemingly minor) will probably need to be transferred for a CT of the head. The timing of the fall, however, may sway the decision on how the patient is transferred for imaging. A recent fall with a loss of consciousness should go by an ALS transport unit. A fall that occurred >24 hours ago in a patient who is oriented and thinking appropriately could be driven by a family member if the patient and their story are reliable.9
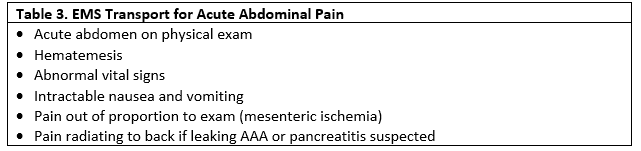
Abdominal Pain
Abdominal pain is a tricky complaint. Our history will get to the bottom of many complaints, and the physical exam may hone the diagnosis with findings of an acute abdomen, bruising, distention, surgical scars, or infection. But vague or long-term abdominal pain with normal vitals are sometimes able to be discharged home or asked to return for serial abdominal exams. A urinalysis is helpful in ruling out ureteral stone and infection of bladder or kidney.
Women of childbearing age should be asked about pregnancy and, when in doubt, a urine pregnancy test will be helpful.
The pregnant patient with acute, severe abdominal pain will require EMS transport to the ED for evaluation for ruptured ectopic pregnancy and other obstetric-related emergencies.
Pain which radiates to the back may be a symptom of leaking abdominal aortic aneurysm (AAA), or pancreatitis or biliary stone.
Some patients will need referral for abdominal imaging if that is not available at the urgent care center. The long-term risk of cancer from computerized tomography is real, so many centers will opt for ultrasound or magnetic resonance imaging (MRI) in some cases. For example, ultrasound may be a first study to consider in evaluating pediatric patients with suspected acute appendicitis.
Acute Change in Mental Status
Acute changes in mental status are most likely due to medical conditions, rather than psychiatric illness, unless the patient has a history of such illness. Overdose of medication (especially opiates) is now so common that it is a first thought in the minds of many EMS providers. Other medical causes of acute mental status change include alcohol intoxication or withdrawal, infection (CNS or sepsis), hypoglycemia, hypoxia, stroke, or occult head trauma. Abnormal vital signs, diaphoresis, or nystagmus are physical signs that point to acute medical illness.

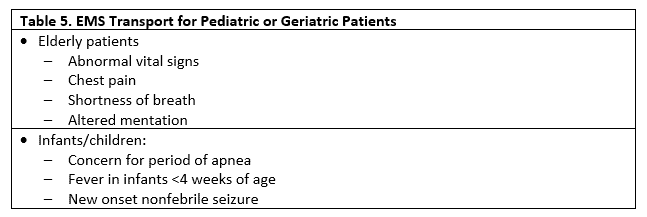
Extremes of Age
Both pediatric and geriatric patients sometimes prove difficult to diagnose. They may display unusual presentations of ordinary problems. History-taking is difficult in very young children, and the elderly with some form of dementia are difficult to evaluate. One helpful clue to medical emergency is an abnormal vital sign. Fever suggests infection; tachycardia suggests circulatory failure or pulmonary embolism, for example. Patients with abnormal vital signs evaluated in the urgent care setting have documented increases in morbidity and mortality.10
Initial Stabilization and Management
Efforts to stabilize the patient in the urgent care center should be performed while awaiting EMS arrival. Although evaluation and treatment will be started and continued by EMS, initiation of treatment in urgent care may make the difference between life and death. Intramuscular epinephrine must be given as soon as possible to patients with anaphylaxis. Nebulized albuterol is given in an acute asthma exacerbation. Administration of aspirin and placement of an intravenous line in a STEMI patient is extremely helpful if the patient develops a life-threatening arrhythmia. Procedures like splinting and bandaging can be completed without delaying transport.
Perhaps the most important act of the urgent care physician is to greet EMS on arrival. Although this may mean interrupting other patients’ visits, it is important to provide EMS with an accurate history and list of treatments to date, as well as help EMS begin treatment and transport as soon as possible.
Emergency Medical Services: Resources and Equipment
EMS brings a lot to the table when they come to transport a patient. If additional personnel or equipment is needed, most EMS systems can request such back-up. Every agency has minor variations. Usually, however, when you request an ALS ambulance you can expect the following:
- Trauma
- Cervical collars
- Tourniquets
- Patient extrication equipment including backboards
- Splinting and dressing supplies
- Intravenous (IV) fluids
- Cardiac
- Cardiac monitoring
- Intravenous fluids, crystalloids, and medications including antiarrhythmic agents and vasopressors
- Pacing/ cardioverting and defibrillating capabilities
- Oxygen
- Respiratory
- Nebulized breathing treatments
- CPAP
- Airways
- Supraglottic devices
- Intubation supplies
- RSI medications in some systems
- Surgical airway
Mode of Transport
The choice between EMS and a personal vehicle cannot be made lightly, and requires consideration of several factors: Is the patient alone? Do they have a reliable driver? Is there a chance the patient may deteriorate? Do the patient and family understand the severity of their illness, and will go straight to the ED?
EMS is a viable option for transport, and is the obvious choice if the patient is unstable or if you are anticipating the patient to deteriorate during transport.
Once you determine the patient needs EMS transport, there are more decisions to be made. There are still regions of the U.S. that may not have ALS ambulance coverage. While most patients will need ALS transport, you may be able to have a basic life support (BLS) crew transport a select few.
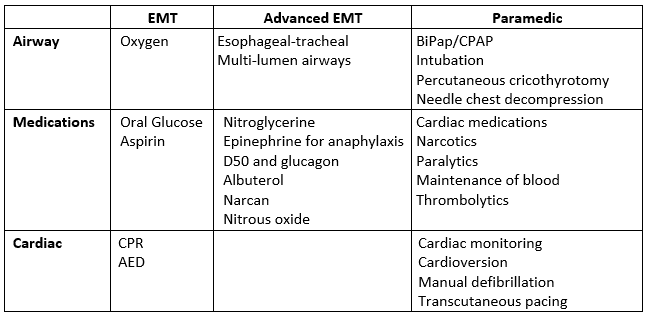
National Registry Emergency Medical Technicians (NREMT) have several categories of certification. Below is a quick overview of the capability of each level by NREMT standards. Different agencies may be able to perform at a higher or lower standard according to their protocol and medical directors’ orders.
Emergency Medical Personnel—Capabilities by Certification11
Ground vs air
Air transport is held in high regard among prehospital EMS. However, it may not be the optimal form of transportation for your patient. When time is a factor and the distance to definitive care is great, this may be the logical choice. There are several points to consider when delineating between air vs ground. Is there a place to land the aircraft, for example? You also have to consider the time for the aircraft to launch and land. In many instances, once you factor this time in, a ground transport is quicker. Also, in many locations the patient will still require a ground EMS unit to transport to the aircraft.
Emergency vs Nonemergent Transport
Does your patient require an emergency transport or nonemergent transport? Along with the patient report, vitals, and interventions you have performed, you should also make EMS aware of expected complications that may arise, and offer suggestions for correcting these if possible. This is when your suggestion for transport mode should be relayed to the crew. Emergency transport should be used only when there would be a possibility of harm to the patient if there was a delay in care. Some instances include unstable vitals, a myocardial infarction, or shortness of breath that cannot be resolved at your facility, or may return prior to arrival at the accepting facility.
Emergency Transfer: Lights and Siren
Use of lights and siren increases the risk of accidents with injury to drivers, EMS personnel, and their patients, and thus is controversial. The risk is particularly high at intersections where drivers may be distracted and not recognize EMS vehicles proceeding through red lights or stop signs.
Lights and sirens are used in two circumstances. The first is in response to an EMS call; the second is in transport of the patient to the hospital. In some studies, use of lights and sirens in response to a 911 call showed minimal effects on response time or patient outcome.12
Not every call requires lights and sirens, but some are clearly time-critical and do require such a response. Call centers that dispatch EMS may use algorithms and protocols that indicate the speed of response needed by EMS. Such priority dispatching determines the need for the use of lights and sirens in response to the call. The content of the information relayed to the call center by urgent care will be critical in determining the response.
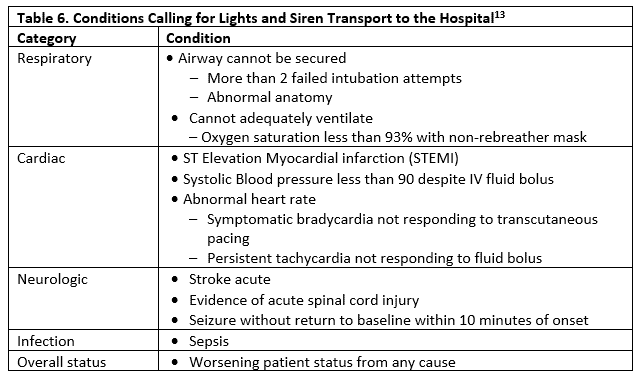
For transport to the hospital, some authors have recommended use of lights and sirens if the conditions listed in Table 6 are present.
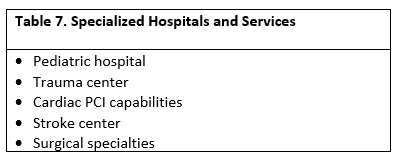
Appropriate Accepting Facility
“You don’t have to go home, but you can’t stay here.” The Oak Ridge Boys may have a good point, but there are several factors that should influence your patient’s destination. While we know that the patient always has the last say in where they go, they also need to be able to make an informed decision. A significant delay in care will occur if a patient is transferred to an inappropriate facility. It would be of little benefit to send an MI to a facility that had no percutaneous coronary intervention (PCI) capabilities, or a patient with an acute stroke to an ED without the ability to at least administer systemic thrombolytic agents if it’s possible to send them to a comprehensive stroke center capable of endovascular intervention.
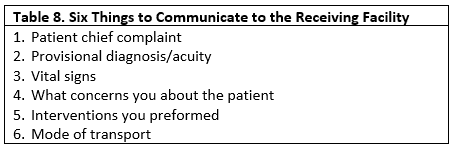
Communicating with the Accepting Facility
Handoffs often result in errors; the lack of face-to-face communication is fraught with challenges. When contacting the accepting facility, we are frequently faced with issues that allow us to leave a less-than-perfect patient report. Not being able to speak to the accepting physician, whether it is you speaking to a transfer center to a generic physician at the accepting facility but who may not be the physician actually taking your patient when they arrive, is a less-than optimal circumstance.14
Communicating to the facility should be a top priority, as this will allow them to understand the acuity of the patient as well as what you are concerned. For example, an elderly patient with a pulsatile abdominal mass and hypotension should be transported emergently with concomitant notification of the ED and/or vascular surgeon. Transfer should not be delayed, but a diagnosis of a likely surgical problem with arrangements for emergent management will improve outcomes.
Call Them Back!
A good way to tie everything together and close the loop of communications is by a second call to the accepting facility an hour after transfer. A call back to the accepting physician allows for a final discussion of your concerns, as well as allows you to answer any questions that may have arose and ensure that the patient did present to the facility if they went by personal vehicle.15
Against Medical Advice
As long as the patient is of sound mind and judgment, they can refuse your recommendations. Even if you believe the patient needs to be seen and treated at another facility, they can elect to end their treatment at your facility. If your patient chooses this, there are several steps that you should take. It is sometimes helpful to have the patient repeat these things back to you verbally, so you know they understand. In addition:
- Attempt to understand why they are refusing. Understanding and discussing their concerns may convince them to continue with your recommendations.
- Explain their condition.
- Explain why you are wanting to transfer them.
- Explain their treatment options and your recommended treatment.
- Explain what could happen if they choose to not have the treatment/transfer.
- Offer alternatives. Just because they refuse a transfer does not mean that you should stop all care (ie, a patient with an infection should still receive a prescription for the appropriate antibiotics).
- Urge them to come back or go to the facility you were planning on transferring them to if they decide to continue care.
- Document all of your discussions thoroughly and have the patient sign an Against Medical Advice (AMA) form.
Conclusion
Transferring a patient is a multifaceted and time-consuming process. There are several areas in which errors can easily arise. Taking care to understand who needs to be transferred, what the appropriate facility is, and how the patient will get there are key components to optimizing the patient’s urgent care experience.
Rogers D, Rund DA. Urgent care transfers: why, when, and how. J Urgent Care Med. March 2018. Available at: https://www.jucm.com/urgent-care-transfers-why-when-and-how/.
References
- O’Cathain A, Knowles E, Maheswaran R, et al. A system-wide approach to explaining variation in potentially avoidable emergency admissions: national ecological study. BMJ Qual Saf. 2014;23(1):47-55.
- Filipiak, KJ, Koltowski L, Grabowski M, et al. Prospective comparison of the 5 most popular risk scores in clinical use for unselected patients with acute coronary syndrome. Circ J. 2011;75(1):167-173.
- Boubaker H, Grissa MH, Beltaief K, et al. A new score for the diagnosis of acute coronary syndrome in acute chest pain with non-diagnostic ECG and normal troponin. Emerg Med J. 2015;32(10):764-768.
- Johnston K, Chapman S, Mehndiratta P, et al. Current perspectives on the use of intravenous recombinant tissue plasminogen activator (tPA) for treatment of acute ischemic stroke. Vasc Health Risk Manag. 2014;10:75-87.
- Maingard J, Churilov L, Mitchell P, et al. Selection criteria for endovascular therapy for acute ischaemic stroke: Are patients missing out? J Med Imaging Radiat Oncol. January 9, 2018. [Epub ahead of print]
- Stiell I, Wells G, Laupacis A, et al. Multicentre trial to introduce the Ottawa ankle rules for use of radiography in acute ankle injuries. Multicentre Ankle Rule Study Group. BMJ. 1995;311(7005):594-597.
- Stiell IG, Wells GA, Vandemheen K, et al. The Canadian CT Head Rule for patients with minor head injury. Lancet.2001;357(9266):1391-1396.
- Hoffman JR, Wolfson AB, Todd K, Mower WR. Selective cervical spine radiography in blunt trauma: methodology of the National Emergency X-Radiography Utilization Study (NEXUS). Ann Emerg Med. 1998;32(4):461-469.
- Nishijima DK, Offerman SR, Ballard DW, et al. Immediate and delayed traumatic intracranial hemorrhage in patients with head trauma and preinjury warfarin or clopidogrel use. Ann Emerg Med. 2012;59(6):460-468.
- Hart J, Woodruff M, Joy E, et al. Association of age, systolic blood pressure, and heart rate with adult morbidity and mortality after urgent care visits. West J Emerg Med. 2016;17(5):591-599.
- National Highway Traffic Safety Administration. National EMS Scope of Practice. Available at: https://www.ems.gov/pdf/education/EMS-Education-for-the-Future-A-Systems-Approach/National_EMS_Scope_Practice_Model.pdf. Accessed February 8, 2018.
- Murray B, Kue R. The use of emergency lights and sirens by ambulances and their effect on patient outcomes and public safety: a comprehensive review of the literature. Prehosp Disaster Med. 2017;32(2):209-216.
- Merlin MA, Baldino KT, Lehrfeld DP, et al. Use of a limited lights and siren protocol in the prehospital setting vs standard usage. J Emerg Med. 2012;30(4):519-525.
- Cheung DS, Kelly JJ, Beach C, et al. Improving handoffs in the emergency department. Ann Emerg Med. 2010;55(2):171-180.
- Propp DA. Improving handoffs in the emergency department. Ann Emerg Med. 2010;56(2):204-205.
Deb Rogers, DO is Junior Chief Resident at Adena Health Systems. Douglas A. Rund, MD, FACEP, FAEMS is Associate Dean of Ancillary Services at The Ohio State University College of Medicine. The authors have no relevant financial relationships with any commercial interests.