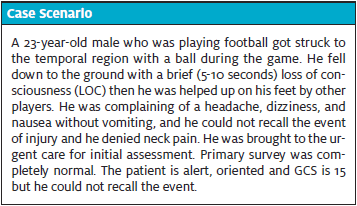
Published on
Urgent message: As visits to urgent care after possible traumatic brain injury continue to rise, so does the importance of understanding which patients require a CT scan. Assessing the value of the Canadian Computed Tomography Head Rule in making that determination can raise the urgent care provider’s ability to make informed decisions in this regard, reducing the risk of unnecessary radiation exposure in patients who are determined to not need a CT.
Jessicah Ray, DHSc, MS, PA-C and Jeffrey L. Alexander, PhD, FAACVPR, ACSM-CEP
Abstract
Background
Despite years of training of emergency department (ED) providers, rates of unnecessary head computed tomography (CT) scans after acute traumatic brain injury continue to increase internationally, exposing patients to unnecessary radiation and increased cancer risk.
Objective
The purpose of this descriptive, cross-sectional, correlational study was to quantify the awareness and use of the Canadian Computed Tomography Head Rule (CCHR) among American urgent care providers and to assess predictor variables of provider characteristics.
Methods
The current study used a modified self-administered online survey that was purposely distributed to active urgent care (UC) providers in the United States. Snowball methods were used to increase distribution. Results were analyzed with descriptive and correlation statistics.
Results
Forty-eight of 70 surveys were analyzed. Twenty-two were rejected for not meeting inclusion criteria (ie, not medical providers) or not answering past the study exclusion questions. Almost half of providers had CCHR awareness (45%) and use rates (43%). They also had highly positive attitudes on the use, applicability, and desired training of the CCHR. Further, CCHR awareness was associated with familiarity with the survey’s clinical case scenario (P=.03, φ=0.34).
Conclusion
The CCHR is an applicable and accepted tool that can be used by urgent care providers as a novel strategy to prevent overuse of head CT scans and decrease patient harm.
INTRODUCTION
Traumatic brain injury (TBI) is a leading cause of global disability and death1 and necessitates continued research to optimize identification and management. Head computed tomography (CT) is the gold standard medical imaging test to identify intracranial hematoma that could require immediate intervention to prevent death or morbidity after acute TBI.2,3 However, radiation from head CT causes the equivalent amount of 8 months of natural radiation exposure, or 115 chest x-rays.4 Notably, more than 80% of TBIs are classified as mild (mTBI or concussion) and rarely require a head CT.1 When CTs are obtained for mTBIs, more than 90% are negative for clinically significant findings, and less than 1% require neurosurgical intervention.5-7 Emergency medicine providers have been the primary audience for training on the appropriate use of medical imaging, but unnecessary head CT rates in the emergency department continue to increase worldwide.8,9
New prevention strategies are needed, and nonhospital providers who refer patients for head CT inappropriately are an ideal and novel target population to reduce overuse of CT.6,10
Overuse of CT is a public health problem; an estimated 12 preventable radiation-induced cancer deaths occur each day in the United States.11 An individual’s estimated increased lifetime cancer risk after a CT is influenced by multivariate factors. Radiation from head CT causes the equivalent amount of 8 months of natural radiation exposure or 115 chest x-rays.12 As global cancer rates increase, judicious limitations on imaging radiation exposure and enhanced clinical discretion are imperative,3,13 especially in pediatric patients who have developing brains, increased radiation sensitivity, and more years to accumulate cancer-causing exposures.3,10 Of CT scans performed, 10% have incidental findings that may result in repeat scans, causing additional radiation exposure.14 Given these outcomes, research does not support the increased use of head CTs.7
To decrease the use of head CT, the Centers for Disease Control and Prevention, in conjunction with the American College of Emergency Physicians, developed clinical recommendations and initiated a TBI-tracking program to reduce unnecessary CTs in mild head injury patients, inform clinical health policy, and improve TBI identification, which is currently at only 11% nationally.15 Electronic clinical tools, such as interactive websites, online training, bedside tablets, mobile applications, and clinical decision prompts, were also developed to decrease unwarranted head CTs.14,16
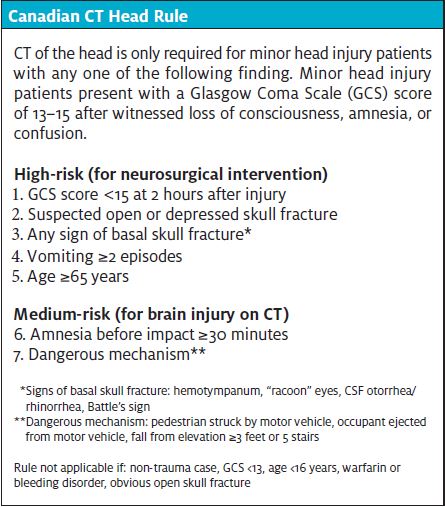
A clinical decision tool (CDT) can be used to guide clinician decisions and involves three or more variables from the history, examination, and simple tests.5 The Canadian Computed Tomography Head Rule (CCHR) is a CDT developed by Stiell, et al17 to guide the ordering of head CT scans for patients with mild head injury. It is considered the most accurate CDT for ruling out the need for head CT by identifying clinically significant findings and cases requiring neurosurgical intervention.18,19 The CCHR is 100% sensitive and has been consistently validated, has a demonstrated superiority over other head injury CDTs, and has shown global applicability and cost effectiveness in most hospital settings.2,3,6,7,13,17,18,20 The CCHR has the potential to decrease head CTs by nearly 40%21,22 and is an effective and easy tool for diverse healthcare providers triaging mild head injuries. It can be beneficial in the urgent care setting when there is no direct access to head CT. Further, research supports its use in multiple specialties.22,23
Over 80% of TBI medical care occurs in the outpatient setting.24 injuries are regularly triaged and stabilized in urgent care centers, where providers frequently have to determine which patients require transfer to the ED or an imaging facility.17,19,25,26 A visit to an urgent care center costs 10% as much as a trip to the ED—and the capabilities of urgent care centers are expanding. Further, urgent care centers outnumber EDs nationwide, and over 150 million patients visit UCs annually.25,27,28
Patients referred to the ED by non-ED providers can increase rates of inappropriate CTs.19,25 Patient demand and a lack of economic deterrents, combined with a cultural perspective that more information is better, has encouraged imaging overuse.14 In nearly 40% of ordered CTs, the patient’s expectation of CT overrode CCHR determinations and influenced inappropriate CT.14,19,29,30 However, research suggests reassuring patients can effectively prevent CT misuse.30
Given the persistent overuse of CT, studies investigating the use of the CCHR should be conducted in broader populations, new settings, and clinical practice.18,20,29,31 To our knowledge, no studies have evaluated the CCHR in an urgent care setting, and only one study examined the CCHR in a non-ED setting.23 Therefore, quantifying urgent care provider awareness and use of the CCHR may highlight this population for targeted interventions to reduce unnecessary CT referrals.19,29,32 In addition, investigating urgent care provider awareness and use of the CCHR may allow UC and ED providers to improve appropriate medical imaging and quality of care by reducing health resource waste, improving patient safety, and decreasing patient harm.8 The purpose of the current study was to quantify the awareness and use of the CCHR among American urgent care providers and to assess predictor variables of provider characteristics.
Methods
The current study used a descriptive, cross-sectional, correlational study design. A modified version of an existing survey was distributed electronically to active urgent care providers in the U.S. Using models from previous studies,2,26,33 we defined study predictor variables as urgent care provider characteristics and dependent variables as awareness and use of the CCHR. All medical providers (osteopathic and allopathic physicians, nurse practitioners, and physician assistants) actively working in an urgent care setting in the U.S. were invited to participate. However, providers were excluded if their urgent care facility had an in-house CT scanner or were attached to an ED that had a CT scanner. Purposeful sampling was used to target urgent care registries, provider organizational platforms, big chain UC managers, and open-access social platforms. Snowball sampling was also used to broaden the sampling pool. TheA.T. Still University-Mesa Institutional Review Board approved the study protocol and waived the need for informed consent.
Survey Development
The study survey was modeled after the data collection tool of Eagles et al33 and included the ED-designed concussion scenario of Bukhari,2 where CT is not indicated. We received permission to use and adapt the data collection tool33 from CCHR developer, Dr. Ian Stiell. For the current study, the demographic and case scenario content were modified to meet our urgent care target population. The data collection tool33 underwent subject matter expert review for content validity and was piloted for internal reliability.
The modified survey assessed clinical judgment for the indication of head CT after mTBI; method of CCHR use and nonuser willingness to use the tool (acceptability); provider attitudes; and provider characteristics modified from the data collection tool33 with additions to meet urgent care demographics.
Data Collection
The study survey was distributed electronically using SurveyMonkey and took about 5-10 minutes to complete. Potential urgent care provider participants were recruited through emails with an invitation letter sent to UC businesses and through posts on social media. No financial incentives were offered for participation. Providers were informed that participation was anonymous, and that aggregate reporting would be used to protect privacy. The survey was available for 10 weeks, and advertisement for participants was continuous during this time with repeated social media posts and reminder emails sent to urgent care chain leadership.
Statistical Analyses
Analyses were conducted using IBM SPSS Statistics version 26.0. Shapiro-Wilk tests for normality were used to report mean and standard deviation or median and interquartile range for ratio level predictor variables. Awareness of the CCHR had a binary response of yes or no in the survey. Urgent care providers who reported they used the CCHR always or most of the time were regarded as users, and those who reported use as sometimes or never were regarded as nonusers. Likert scale questions were scored to determine the primary promoters and barriers for use by CCHR user or nonuser groups based on the level of agreement or disagreement with each of 11 statements about the CCHR.
To determine which predictor factors of provider characteristics were associated with awareness and use of the CCHR, χ2 tests for association were used. Raw numerical data (such as age and number of head injuries evaluated per month) were converted into ranks, and ordinal data were converted to nominal variables to meet χ2 assumptions.
Results
Urgent Care Provider Characteristics
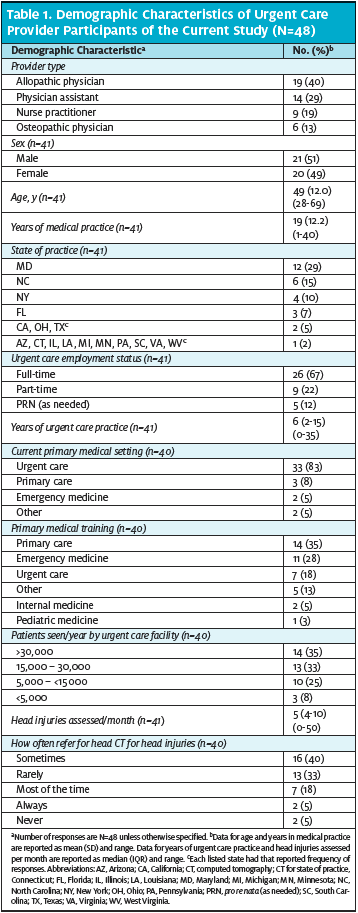
Of the 70 respondents who participated in the online survey, 48 were included in our analysis. Twenty-one surveys were excluded because they did not meet inclusion criteria and one because the respondent did not complete the survey beyond the first four questions. The urgent care provider demographic characteristics are presented in Table 1.
Likert Scale Questions
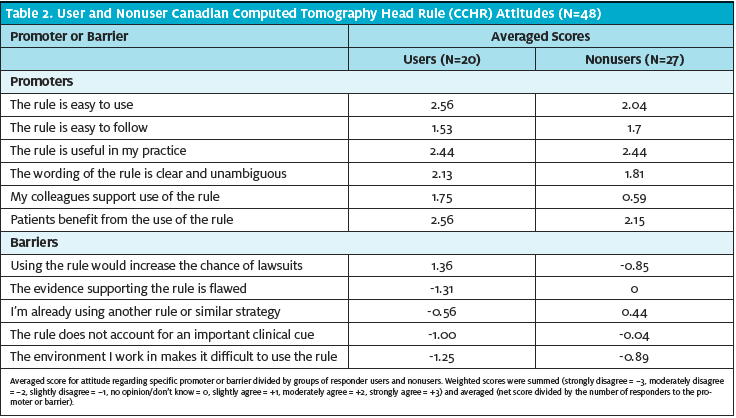
Overall, urgent care provider responses to Likert scale questions were positive for use of the CCHR (Table 2). Scores showed moderate agreement for the six promoters and mostly slight disagreement for the five barriers. Users and nonusers had consistent responses for the top three promoters: the rule is useful in my practice, patients benefit from the use of the rule, and the rule is easy to use. Of all grouped promoter scores possible, a predominant promoter was identified by nonusers: the CCHR is useful in their practice. The urgent care providers disagreed with all barriers, although nonusers generally agreed with the barrier of using another rule or similar strategy; there was also a neutral response score for the evidence supporting the rule is flawed.
Correlational Results
When analyzing which predictor factors of provider characteristics were associated with awareness and use of the CCHR, awareness was associated with familiarity with the clinical case scenario.
Case Scenario
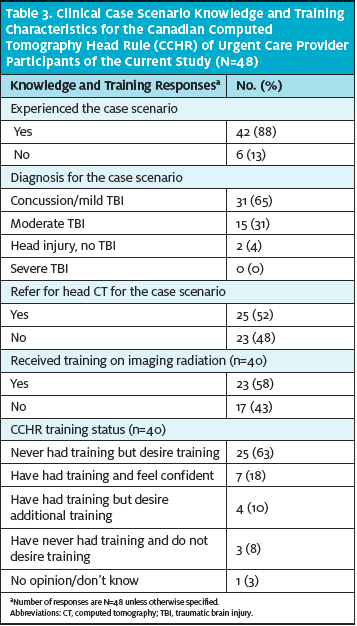
Most providers (42/48, 88%) were clinically familiar with the case scenario (Table 3). When diagnosing the scenario, 65% (31/48) correctly identified the mTBI, yet 52% (25/48) incorrectly chose to refer for head CT. Over half (23/40, 58%) had received training on medical imaging radiation, and most (29/40, 73%) indicated interest in new or renewed CCHR training.
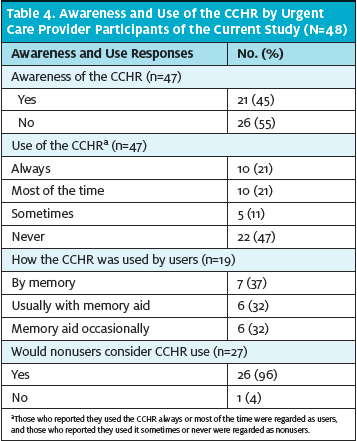
Awareness and Use
Slightly less than half of urgent care providers (21/47, 45%) were aware of the CCHR (Table 4). Users of the CCHR (20/47, 43%) used the tool similarly. Of nonusers, all but one (26/27, 96%) would consider using the CCHR.
Discussion The current study assessed the awareness and use of the CCHR among urgent care providers and predictor variables of provider characteristics using an electronic survey distributed to active urgent care providers in the U.S. We surveyed urgent care providers because they regularly assesses acute head injuries and may contribute to overuse of CT. Slightly less than half of urgent care providers were aware of (45%) or used (43%) the CCHR, which was higher than previously reported awareness (31%) and use (12%) rates by ED providers in the U.S.33 However, the previous international study33 of ED providers (Australia, Canada, United Kingdom, and United States) had more participants (N=1297), with 239 ED providers from the U.S., which may explain the discrepancy (Table 5).
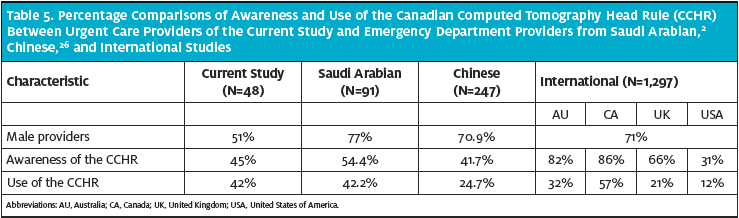
Results for the international providers tended to have higher CCHR awareness (range, 66%-86%), but results for use of the CCHR were more varied (range, 21%-57%).33 A study of Saudi Arabian ED providers2 found awareness (54%) and use (42%) rates similar to the current study. Awareness results from a Chinese study were also similar (42%).26
The current study also found urgent care providers overall had positive attitudes about the CCHR. Further, the acceptability by nonusers of the CCHR was higher among our urgent care providers (96%) than ED providers in the United States (63%).33 Higher reported awareness, use, and acceptability of the CCHR among urgent care providers supports allocation of resources for targeted CCHR training in the UC setting that may otherwise be reserved for ED providers.
Most urgent care providers in the current study were clinically familiar with the case scenario, which suggested the addition of this ED-designed concussion scenario where CT is not indicated is pertinent for urgent care providers. However, even though most providers were familiar with head injury assessment, only 65% correctly identified the mTBI, and over half incorrectly referred for an unnecessary head CT, despite having received training on medical imaging radiation. When analyzing predictor factors, awareness of the CCHR was associated with familiarity with the case scenario.
Taken together, these results suggested that providers who reported awareness, training, or even use of the CCHR could still be misusing head CT.
Perhaps one reason for this outcome is cultural inertia acting as a barrier to CDT implementation even when awareness of these tools is high.23,33 Therefore, more education and outreach programs are necessary to teach urgent care providers about the proper use of the CCHR and reduce use of CT. Despite years of targeted ED provider training, the rarity of CT indication for mild head injury, and the sensitivity and wide applicability of the CCHR, the inappropriate use of CT continues to increase worldwide, causing unnecessary patient harm and death.2,4,8,14,22,32 Overuse of CTs by CCHR-trained ED providers has been associated with barriers of provider insecurities, litigation fear, peer or leadership pressure to order CT, lack of awareness of the radiation harm from CTs, and patient expectation or demand for CTs.19,26,30 These insecurities overtax healthcare funds, decrease patient safety, and reduce provider confidence in clinical decision-making.20 Unfortunately, literature regarding use of the CCHR seems to mostly focus on ED providers even though components of the tool apply to a variety of medical professionals who triage head injuries, such as athletic trainers, medics, and others.34-36 Therefore, awareness and use of the CCHR should be expanded to broader populations of healthcare providers, new settings, and clinical practice.10,18,20,29
The importance of increasing awareness and use of the CCHR among urgent care providers cannot be stressed enough. Importantly, urgent care facilities offer timely medical care at a fraction of the cost of EDs.25,27,28 Since most urgent care facilities lack CT scanners, those that triage and stabilize head injuries should use the CCHR to determine which patients actually require transfer to the ED for CT.17,19,26,27 Remarkably, research suggests that when patients are reassured about the CCHR the misuse of CT can be prevented.15,30 Therefore, patient health and safety can be protected by training urgent care providers to use the CCHR to reinforce clinical decisions and to educate patients about why CT is not indicated. Keeping patient care at the urgent care level when a diagnosis of concussion (mTBI) is more likely may encourage the education and reassurance necessary for optimal outcomes.17,23
The use of the CCHR also provides practical applications over medical devices. For instance, the clinical device market for acute TBI assessment has increased in recent years. However, the physical exam conducted during use of the CCHR supports the initial neurological exam, both of which narrow the differential diagnosis better than a TBI digital device. In addition, no TBI devices currently have 100% sensitivity identifying head CT indications.37 So, because CTs have been used as a surrogate for clinical examination in the ED setting,14,38 the temptation to substitute the physical exam for an unnecessary, expensive, and less informative test is real and should be a concern for all healthcare providers.
Limitations
The current study had several limitations. We only assessed the awareness and use of the CCHR among urgent care providers in the U.S., so the generalizability of our results is limited. Also, we did not ask about the use of other head triage guidelines or CDTs, such as the Clinical Practice Guideline for Management of Concussion/Mild Traumatic Brain Injury39 or the New Orleans Criteria for CT scanning.40 However, nonusers of the current study identified use of another tool as a barrier to CCHR use, which may explain our results for that outcome.
Since the survey was self-administered, another limitation is self-report bias. However, participating urgent care providers were assured of their anonymity, and we used aggregate reporting to decrease self-report bias. Because we used snowball distribution of the survey, we could not determine participant nonresponse rate or perform a response bias analysis.
Another limitation is that our sample size was small, and we had some incomplete surveys. Therefore, our correlational analyses were unable to address the original research questions about associated characteristics.
A better understanding of the specific barriers and promoters of the awareness and use of the CCHR among urgent care providers in the U.S. (and worldwide) may lead to more effective education, training, and resource allocation. As a result, urgent care providers would be better equipped to use informed clinical decisions regarding head CT for acute mTBI. Additional studies of CCHR use among urgent care providers should be conducted.
Conclusion
A driving goal of the current study was to acknowledge urgent care providers as vital partners in the U.S. healthcare system and to recognize the CCHR as a valuable and practical tool for head injury triage, assessment, and management in the UC setting. The current study demonstrated applicability of the CCHR in the urgent care setting as well as high UC provider CCHR awareness, use, and acceptability. However, most urgent care providers reported overuse of head CT, indicating the need for CCHR training to improve proper use and adherence. Results of the current study suggested the CCHR can be immediately adopted by urgent care providers as a key clinical tool to guide clinical decisions, reassure patients, and prevent harm.
References
1. Centers for Disease Control and Prevention. Traumatic brain injury and concussion. https://www.cdc.gov/traumaticbraininjury/index.html. Accessed June 2, 2020.
2. Bukhari H. Emergency physicians awareness of computed tomography indication in traumatic brain injury: a questionnaire-based study. Open J Emerg Med. 2017;5(3):93-101.
3. Cellina M, Panzeri M, Floridi C, et al. Overuse of computed tomography for minor head injury in young patients: an analysis of promoting factors. Radiol Med. 2018;123(7):507-514.
4. Radiation dose in x-ray and CT exams. RadiologyInfo.org website. https://www.radiologyinfo.org/en/info.cfm?pg=safety-xray. Accessed June 2, 2020.
5. Clement CM, Stiell IG, Schull MJ, et al. Clinical features of head injury patients presenting with a Glasgow Coma Scale score of 15 and who require neurosurgical intervention. Ann Emerg Med. 2006;48(3):245-251.
6. Sadegh R, Karimialavijeh E, Shirani F, et al. Head CT scan in Iranian minor head injury patients: evaluating current decision rules. Emerg Radiol. 2016;23(1):9-16.
7. Smits M, Dippel DW, de Haan GG, et al. External validation of the Canadian CT Head Rule and the New Orleans Criteria for CT scanning in patients with minor head injury. JAMA. 2005;294(12):1519-1525.
8. Sharp AL, Huang BZ, Tang T, et al. Implementation of the Canadian CT Head Rule and its association with use of computed tomography among patients with head injury. Ann Emerg Med. 2018;71(1):54-63 e52.
9. Stiell IG, Clement CM, Grimshaw JM, et al. A prospective cluster-randomized trial to implement the Canadian CT Head Rule in emergency departments. CMAJ. 2010;182(14):1527-1532.
10. Klora M, Zeidler J, Bassler S, et al. Frequency of neuroimaging for pediatric minor brain injury is determined by the primary treating medical department. Medicine (Baltimore). 2019;98(28):e16320.
11. Smith-Bindman R, Lipson J, Marcus R, et al. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch Intern Med. 2009;169(22):2078-2086.
12. Mahesh M. Computed tomography dose (CT dose). RadiologyInfo.org. Available at: https://www.radiologyinfo.org/en/info.cfm?pg=safety-xray. Accessed November 9, 2020.
13. Zyluk A. Indications for CT scanning in minor head injuries: a review. Neurol Neurochir Pol. 2015;49(1):52-57.
14. Swensen SJ. Patient-centered imaging. Am J Med. 2012;125(2):115-117.
15. American College of Emergency Physicians. Five things physicians and patients should question. Choosing Wisely website. http://www.choosingwisely.org/wp-content/uploads/2015/02/ACEP-Choosing-Wisely-List.pdf. Accessed June 2, 2020.
16. Singh N, Hess E, Guo G, et al. Tablet-based patient-centered decision support for minor head injury in the emergency department: pilot study. JMIR Mhealth Uhealth. 2017;5(9):e144.
17. Stiell IG, Wells GA, Vandemheen K, et al. The Canadian CT Head Rule for patients with minor head injury. Lancet. 2001;357(9266):1391-1396.
18. Bouida W, Marghli S, Souissi S, et al. Prediction value of the Canadian CT head rule and the New Orleans criteria for positive head CT scan and acute neurosurgical procedures in minor head trauma: a multicenter external validation study. Ann Emerg Med. 2013;61(5):521-527.
19. Curran JA, Brehaut J, Patey AM, et al. Understanding the Canadian adult CT head rule trial: use of the theoretical domains framework for process evaluation. Implement Sci. 2013;8:25.
20. Anish TS, Sreelakshmi PR, Medhavan S, et al. Efficacy of Canadian Computed Tomography Head Rule in predicting the need for a computed-axial tomography scans among patients with suspected head injuries. Int J Crit Illn Inj Sci. 2012;2(3):163-166.
21. Sharp AL, Nagaraj G, Rippberger EJ, et al. Computed tomography use for adults with head injury: describing likely avoidable emergency department imaging based on the Canadian CT Head Rule. Acad Emerg Med. 2017;24(1):22-30.
22. Klang E, Beytelman A, Greenberg D, et al. Overuse of head CT examinations for the investigation of minor head trauma: analysis of contributing factors. J Am Coll Radiol. 2017;14(2):171-176.
23. Zakhari R, Sterrett SE. Attitudes toward evidence-based clinical decision support tools to reduce exposure to ionizing radiation: the Canadian CT Head Rule. J Am Assoc Nurse Pract. 2016;28(12):659-667.
24. Centers for Disease Control and Prevention. CDC’s report to Congress on traumatic brain injury epidemiology and rehabilitation: recommendations for addressing critical gaps. https://www.cdc.gov/traumaticbraininjury/pdf/TBI_Report_to_Congress_Epi_and_Rehab_Snapshot-a.pdf. Accessed June 2, 2020.
25. Ashton LM. Urgent care: a growing healthcare landscape. Nursing. 2017;47(7):21-24.
26. Huang X, Zhou JC, Pan KH, Zhao HC. Awareness and use of the Canadian Computed Tomography Head Rule for mild head injury patients among Chinese emergency physicians. Pak J Med Sci. 2013;29(4):951-956.
27. Ho V, Metcalfe L, Dark C, et al. Comparing utilization and costs of care in freestanding emergency departments, hospital emergency departments, and urgent care centers. Ann Emerg Med. 2017;70(6):846-857. e843.
28. Saidinejad M, Paul A, Gausche-Hill M, et al. Consensus statement on urgent care centers and retail clinics in acute care of children. Pediatr Emerg Care. 2019;35(2):138-142.
29. Davey K, Saul T, Russel G, et al. Application of the Canadian Computed Tomography Head Rule to patients with minimal head injury. Ann Emerg Med. 2018;72(4):342-350.
30. Melnick ER, Shafer K, Rodulfo N, et al. Understanding overuse of computed tomography for minor head injury in the emergency department: a triangulated qualitative study. Acad Emerg Med. 2015;22(12):1474-1483.
31. Jagoda AS, Bazarian JJ, Bruns JJ, Jr., et al. Clinical policy: neuroimaging and decisionmaking in adult mild traumatic brain injury in the acute setting. Ann Emerg Med. 2008;52(6):714-748.
32. Tan DW, Lim AME, Ong DY, et al. Computed tomography of the head for adult patients with minor head injury: are clinical decision rules a necessary evil? Singapore Med J. 2018;59(4):199-204.
33. Eagles D, Stiell IG, Clement CM, et al. International survey of emergency physicians’ awareness and use of the Canadian Cervical-Spine Rule and the Canadian Computed Tomography Head Rule. Acad Emerg Med. 2008;15(12):1256-1261.
34. Tactical combat casualty care. Next Generation Combat Medic website. https://nextgencombatmedic.com/tccc/. Accessed June 2, 2020.
35. Echemendia RJ, Meeuwisse W, McCrory P, et al. The Sport Concussion Assessment Tool 5th Edition (SCAT5): background and rationale. Br J Sports Med. 2017;51(11):848-850.
36. McCrory P, Meeuwisse W, Dvorak J, et al. Consensus statement on concussion in sport: the 5th International Conference on Concussion in Sport held in Berlin, October 2016. Br J Sports Med. 2017;51(11):838-847.
37. Ayaz SI, Thomas C, Kulek A, et al. Comparison of quantitative EEG to current clinical decision rules for head CT use in acute mild traumatic brain injury in the ED. Am J Emerg Med. 2015;33(4):493-496.
38. Tavender EJ, Bosch M, Gruen RL, et al. Understanding practice: the factors that influence management of mild traumatic brain injury in the emergency department: a qualitative study using the Theoretical Domains Framework. Implement Sci. 2014;9:8.
39. US Department of Veterans Affairs, US Department of Defense. VA/DoD Clinical Practice Guideline for the Management of Concussion/Mild Traumatic Brain Injury. Available at: https://www.healthquality.va.gov/guidelines/Rehab/mtbi/mTBICPGFullCPG50821816.pdf. Accessed June 2, 2020.
40. Haydel MJ, Preston CA, Mills TJ, et al. Indications for computed tomography in patients with minor head injury. N Engl J Med. 2000;343(2):100-105.
Author affiliations: Jessicah Ray, DHSc, MS, PA-C, College of Graduate Health Studies, A.T. Still University, Mesa, AZ. Jeffrey L. Alexander, PhD, FAACVPR, ACSM-CEP, College of Graduate Health Studies, A.T. Still University, Mesa, AZ. The authors have no relevant financial relationships with any commercial interests.